
INTRODUCTION
At the end of last year, we produced a ‘Horizon Scan’ of the disease (and wider personal injury) market for 2020, which predicted the key topics that were expected to dominate legal news headlines over the past 12-months.
In the course of this feature article, we reflect on the past year of published articles in BC Disease News and assess the extent to which our predictions were correct.
Whilst carrying out this exercise, we also re-scan the disease market for any themes that we believe will recur in 2021.
For many months now, the COVID-19 disease pandemic has had a significant impact on all aspects of professional and personal lives. This is something that we could not have anticipated when we published our ‘Horizon Scan’ in 2019.
In the same vein as last year, we separate this feature article into distinct parts:
- A ‘Horizon Scan’ of pre-eminent and emerging disease risks and claims strategies, separated by exposure type.
- A ‘Horizon Scan’ of new-fangled COVID-19 infection claims.
- A ‘Horizon Scan’ of new trends involving aspects of civil procedure, parliamentary affairs and the work of the Ministry of Justice (MoJ).
PART 1 – EMERGING RISKS BY EXPOSURE TYPE
ORGANOPHOSPHATES
Aerotoxic Syndrome
‘Aerotoxic syndrome’ is an as-yet unrecognised medical condition, which is allegedly caused by cumulative exposure to toxic organophosphates in aircraft cabin air (sourced from jet engine ‘bleed air’ supply), during ‘fume events’.
Such contaminants include volatile organic compounds (VOCs), low molecular weight organic acids, esters, ketones, and organophosphates, e.g. tricresyl phosphate (TCP).
The proposed ‘bleed air’ mechanism, by which toxic air apparently enters aircraft, is best described by the diagram, below.
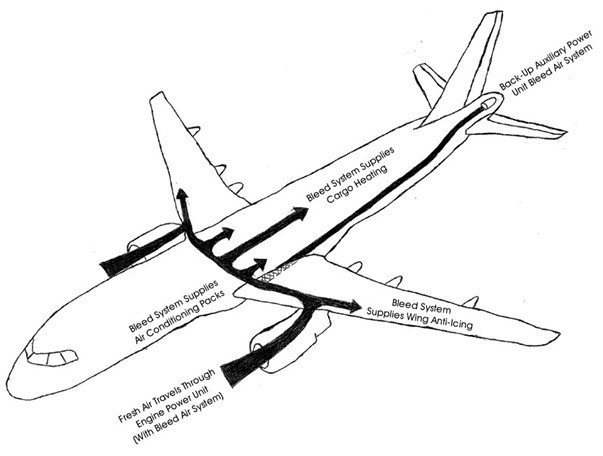
‘Bleed air’ systems are installed on all commercial aircraft, except Boeing 787 Dreamliners.
It is alleged that ‘aerotoxic syndrome’ poses a risk to pilots, cabin crew and frequent flyers on aircraft (besides Boeing 787’s), who may be repeatedly exposed to contaminated air. British Airways (BA), alone, employs 16,500 cabin crew and 3,900 pilots, so the scale of potential liability is vast.
Symptoms of ‘aerotoxic syndrome’ in those who claim to have been cumulatively exposed, include:
- Adverse neurological symptoms (breathing and vision problems);
- Chronic fatigue;
- Memory impairment;
- Cognitive difficulties; and
- An inability to focus or concentrate.
One of the first presumed victims of the so-called syndrome was BA pilot, Richard Westgate, who died aged 43, in 2012, though the result of the inquest into his death revealed that sedative overdose was the underlying cause.
In spite of this, we reported, last year, that Mr. Westgate’s estate had sought a group litigation order, grouping together tens of former pilots and cabin crew (dubbed the ‘Aircraft Cabin Air Litigation’) against the likes of BA, EasyJet, Thomas Cook, Virgin Atlantic and Jet2. Judge Barbara Fontaine, who made the order for collective case management, specified that up to 8 cases, including Mr. Westgate’s case, would return to Court for a full trial.
Although our ‘Horizon Scan’ in 2019 predicted that we would know more by now about the progress of proceedings, currently, we do not. Nor can we inform our readers that Unite’s call for a full public inquiry into ‘aerotoxic syndrome’ has been authorised by the UK Government, or that Belgian research into the neurotoxic effects of aircraft cabin air on 50 ‘(ex-) cabin crew members and (ex-) pilots’ has been concluded.
We do, however, know that prospective litigants with suspected ‘aerotoxic syndrome’ will have been buoyed by news reports at the end of July 2020, that JetBlue pilot, Captain Myers, was awarded compensation following an ‘acute toxic inhalation’ event on an Airbus aircraft, in 2017, which left him with toxic encephalopathy, neuro-cognitive disorder and visual problems.[1]
This is the suspected to have been the 1st case in the US to establish that the fumes that the pilot was exposed to were injurious, albeit the decision was made by a state Workers’ Compensation Board as opposed to high calibre High Court Justices in England and Wales.
Nonetheless, the case was dubbed ‘groundbreaking’ and a ‘great step forward’ for the ‘Aircraft Cabin Air Litigation’.[2]
Reacting to the US ruling, Unite’s Assistant General Secretary for Legal Services, Howard Beckett, stressed that:
‘Unite will use every avenue, including calling for a public inquiry and pursuing legal action, to get the airline industry to take responsibility and clean up the cabin air on jet planes.
This must include using different oils to lubricate jet engines, better monitoring of cabin air, installing air filters and manufacturing planes that bring compressed air straight from the atmosphere’.[3]
Glyphosate Weedkiller
In June of this year, Bayer agreed to settle product liability claims involving glyphosate weedkiller, in the sum of $10.9 billion.[4]
Adjudged to be taking the ‘right action at the right time’, Bayer’s CEO, Werner Baumann, stated that the settlement brokered would ‘bring closure to approximately 75%’ of the current 125,000 filed and unfiled future claims.
Bayer acquired Roundup pesticide manufacturer, Monsanto, in June 2018 – and with it, the liabilities of the company.
For a long time, it has been alleged that glyphosate, the active ingredient in Monsanto-produced weedkillers, is carcinogenic.

[Source: Flickr – Mike Mozart (30 April 2016): ‘Roundup, Monsanto’]
Specifically, it has been purported that prolonged exposure can cause non-Hodgkin lymphoma (cancer of the lymphatic system), as well as onset chronic kidney and liver disease.
As a result, those estimated to be most at risk include:
- Farmers,
- Gardeners;
- Landscapers; and
- Local Government Workers.
Up until June, cases had been ‘vigorously’ defended and as a result, it is not to be presumed that the mammoth US settlement is akin to an admission of guilt or wrongdoing.
Glyphosate is still licensed for sale and use as a Plant Protection Product (PPP) in the EU, until 15 December 2022, and applications for license renewal have been ongoing. That being said, B&Q removed Roundup from its shelves in May, apparently owing to safety concerns posited in US litigation.[5]
France, Hungary, the Netherlands and Sweden were appointed as joint ‘rapporteurs’ [the Assessment Group on Glyphosate (AGG)] for the next glyphosate assessment. This is followed by a peer-review process, overseen by the European Food Safety Authority (EFSA).
In light of events this summer, we feel that it is more likely than ever before that glyphosate-induced non-Hodgkin lymphoma claims could migrate to the UK in significant volumes, whether in an EL/PL context or otherwise.
ASBESTOS
Talcum Powder
Having frequently reported on talc-related product liability claims for the bulk of 2019, often in tandem with glyphosate claims, it will perhaps be surprising to many of our readers that these emerging risks were so often absent from BC Disease News editions in 2020, contrary to what last year’s ‘Horizon Scan’ might have implied.
A large part of this is because Johnson & Johnson has employed the same unforeseen strategy as Bayer – compromise a large number of claims to avoid strung-out court battles.
However, several months prior to agreeing a $100 million settlement figure in October of 2020,[6] in respect of 1,000 product liability lawsuits (there are currently said to be around 21,800 cases pending[7]), the pharmaceutical giant announced that it would no longer be supplying new batches of talcum powder products for US and Canadian shelves.[8]

[Source: Wikimedia Commons – Austin Kirk (26 February 2014): ‘Johnson's Baby powder, 2014’]
Whether or not the catalyst for this decision was the impact of the COVID-19 pandemic on sales, the scale of mounting litigation, the ‘constant barrage’ of litigation advertising, or pressure induced by last year’s voluntary recall of 33,000 bottles of Johnson’s Baby Powder (lot #22318RB) ‘out of an abundance of caution’ [the US Food and Drug Administration (FDA) detected sub-trace levels (no greater than 0.00002%) of chrysotile asbestos in a single sample], it is curious that J&J has stuck with its decision to continue selling talc-containing consumer products in the UK and the rest of the world.[9]
Or, perhaps not so curious, given that J&J has persisted in defending claims based on ‘steadfast confidence’ in the safety of its products, citing ‘decades’ of supportive science and ‘routine testing’. Indeed, the company has consistently overturned unfavourable mesothelioma and ovarian cancer verdicts on appeal, refuting claims that it has known, from at least 1971 until the early 2000’s, that its products were laced with asbestos and therefore defective. Further, that it failed to disclose this fact to regulators or to the public – see the landmark Special Report (2018), conducted by The New York Times and Reuters.
At present, J&J is attempting to appeal its most expensive loss at the US Supreme Court.[10]
In 2018, J&J was ordered to pay $4.69 billion in a combined suit of 22 women with ovarian cancer. This summer, the Missouri Court of Appeals for the Eastern District lowered the verdict to $2.11 billion. J&J was then refused its request for an appeal to the state’s Supreme Court.
Determined to challenge this verdict, which was grounded on a ‘fundamentally flawed trial … in a faulty presentation of the facts’, it will be intriguing to see whether the highest court in the land will choose to review this case in 2021. The US Supreme Court commonly receives around 7,000 applications every year and only takes on 100 to 150.
For British claimants, who may be more tempted than ever to bring a claim now J&J has shown an inclination to settle in bulk, claimant firm, Leigh Day, recently reported that the New York Supreme Court was allowing 45-year-old British woman, Hannah Fletcher, to file a talc-related mesothelioma claim in the US, against Estée Lauder, Avon, and Macys.
Ultimately, the Court held that:
- Although the claimant resides in England, the defendants are located in New York.
- ‘Defendants’ products were developed, manufactured, distributed and/or supplied from New York to England’.
- Defendants would face no hardship litigating in New York.
- The claimant would face significant hardship as the case could not proceed in England.
- The potential need to apply English law did not phase New York Court, which are regularly called on to apply foreign law.[11]
De Minimis Asbestos Exposure?
In May of this year, David Platt QC successfully defended a mesothelioma claim, on the basis that a single incident of asbestos exposure, whose total dose burden was 0.0004 fibre/ml years, was de minimis.[12]
Relying on epidemiological literature and regression analysis [Hodgson & Darnton (2000)], it was predicted that the claimant’s dosage of exposure would produce a lifetime risk of 0.2 deaths per 100,000, or an annual risk of 1:50,000,000.
Mr. Tattersall QC, the Deputy High Court Judge who presided over the case of Bannister (Estate of) v Freemans Public Ltd Company [2020] EWHC 1256 (QB), clarified how ‘materiality’, under the ‘material increase in risk’ (Fairchild[13]) test, is to be determined:
‘… a dose of asbestos which was properly capable of being neglected could be defined as a dose which a medical practitioner who is aware of the medical risks would define as something that the average patient should not worry about’ – Dr. Rudd’s formulation transposed from his answers under cross-examination, in the case of Sloper v Lloyds Bank Plc [2016] EWHC 483 (QB).
In our ‘Horizon Scan for 2022’, will we find ourself citing cases that operate Bannister in acceptance or rejection of this new de minimis threshold test?
Asbestos in Education and Healthcare Settings
In last year’s ‘Horizon Scan’, we presaged that asbestos harboured in school and hospital buildings could be responsible for delaying the downward trend of annual occupational mesothelioma mortality, documented by HSE’s industrial fatality statistics.
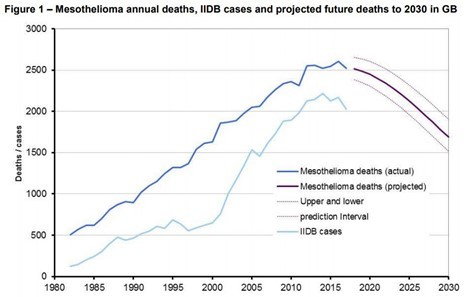
However, in edition 310 (here), we publicised that 80 fewer workers (2,446) died from mesothelioma in 2018 (the most up-to-date reporting year) than in 2017, which could infer a general reduction in exposure to asbestos-containing materials over time.
Indeed, the latest Office for National Statistics (ONS) data on mesothelioma deaths among teaching and educational professionals, up to 2019, would appear to support this presumption.

Irrespective of the seemingly flattening mortality curve, the Education and Skills Funding Agency (EFSA) and the Joint Union Asbestos Committee (JUAC) assert that 80% of schools still contain asbestos and that the risk of asbestos-related disease is ever-present.
Of these schools, around 3,000 were designed in the late 1950’s, under the Consortium of Local Authorities Special Programme (CLASP), with asbestos-containing structural support columns and an intended lifespan of 40-years.
The fact that so many CLASP schools are still standing has been flagged as a matter for concern by Conservative party politician, David Morris MP, who stated earlier this year that the demolition of 1,000 active CLASP buildings would make a ‘considerable difference to the asbestos risk posed by the UK’s total building stock’.
Whether or not ‘well protected’ asbestos continues to be left in-situ and in ‘good condition’ in schools will depend (at least in-part) upon how the funds of a new, £1 billion, ‘transformative’, school 10-year rebuilding programme are divested – read our full report in edition 311 (here).
In next year’s ‘Horizon Scan’, will we write that the Government has caved into the of the National Education Union’s (NEU) Comprehensive Spending Review request, calling for earmarked funding for the ‘phased removal’ of asbestos from all educational buildings in the UK’s 32,770 schools?
Joint and Several Liability in Reinsurance ‘Spiking’
In edition 271 of BC Disease News, we summarised the Court of Appeal’s judgment in Equitas Insurance Limited v Municipal Mutual Insurance Limited [2019] EWCA Civ 718.
The upshot of this landmark decision was that the employers’ liability (EL) insurer (MMI) could not allocate 100% of its liability (in an action called ‘spiking’) to a chosen year of reinsurance cover in an asbestos-related disease claim.
The position between EL insurers and reinsurers is noticeably different from the relationship between employers and EL insurers, where the Fairchild principle applies – see Zurich Insurance PLC UK Branch v International Energy Group Ltd (Rev 2) [2015] UKSC 33. The nature of liability was distinguished because there was a ‘seriously arguable case for treating the insurance and reinsurance positions differently’.
This year, we were expecting Equitas to reach the Supreme Court – an observation we made in last year’s ‘Horizon Scan’.
However, in edition 310 (here), we reported that the parties had settled proceedings, thus confirming the Court of Appeal decision as the established guiding authority for insurers’ ability to ‘spike’ reinsurers under excess of loss liability reinsurance policies.
‘Spiking’, for now at least, is prohibited. EL insurers must present EL asbestos claims to reinsurers on a pro rata, time on risk basis.
NOISE
Opportunistic Applications for Own Engineering Evidence in Spite of SJE Report
An emerging strategy in fast-track industrial disease litigation, this year, has been claimant parties seeking their own engineering evidence in noise-induced hearing loss (NIHL) claims, where a single joint expert (SJE) has already been agreed, instructed and published a report/answered Part 35 questions.
Opportunistic applications have been tactically advanced in instances where a SJE indicates that a claimant’s occupational noise exposure was not excessive – an observation which is terminal to arguments on breach of duty.
In edition 307 (here), we reported that we were handling several cases where such applications had been made and listed to be heard before County Court judges.
At that point in time, we were prepared for this to become a new characteristic of NIHL claims handling, as claimant firms tried their luck at adducing expert evidence from new acoustic engineers by seeking to vacate existing trial dates, seeking reallocation to the multi-track and seeking permission to rely on new reports.
However, in edition 313 (here), we summarised the High Court’s judgment in Hinson v Hare Realizations Ltd (2) [2020] EWHC 2386 (QB), which considered the established case authorities on this issue and found in favour of the defendant.
At first instance, the Recorder assessed the ‘balance of grievance’, were the claimant not to be permitted to rely on their own engineering evidence – the test laid out in Bulic v Harwoods & Ors [2012] EWHC 3657 (QB):
‘… the claimant will be aggrieved at not being able to rely on evidence which might enable him to win his case; but the defendant will also have a strong sense of grievance if this low value case is adjourned for the third time, on the date of trial, with the inevitability of the defendant incurring further very considerable costs, where the single joint expert was proposed by the claimant and where her evidence may well be preferred to that of [the claimant’s own expert] if the case went to trial’.
On appeal to the High Court, Mr. Justice Spencer was not convinced that the lower court decision was an ‘erroneous one’, not least because the SJE boasted ‘appropriate expertise from a well-known firm of experts’.
In line with Lord Woolf, in Daniels v Walker [2000] EWCA Civ 508, who stated that permission to obtain the desired new expert evidence could be permitted for ‘reasons which are not fanciful … subject to the discretion of the court’, Spencer J found that Recorder McNeill QC had acted ‘well within the generous ambit of her discretion’.
Post-Hinson, we have seen some signs of claimant applications being rejected by County Court judges, which is only to be expected if the only reason why own engineering evidence is acquired is to sway the unfavourable opinion of a SJE.
We will resume our interest in this claimant ploy after the winter break.
Hearing Loss in the Music and Entertainment Industry
Following on from the Court of Appeal’s ruling in Goldscheider v Royal Opera House Covent Garden Foundation [2019] EWCA Civ 711, in which a violist was successful in bringing an ‘acoustic shock’ claim against his former orchestral employer, we presumed that there could be significant ramifications for the NIHL market.
Firstly, because ‘acoustic shock’ was accepted, for the first time, as being a ‘relatively new’ and ‘albeit developing’ medical phenomenon that does not exclusively affect call centre workers exposed to white noise through earpieces or telephone speakers.
Secondly, and arguably most importantly, because it created binding legal precedent that noise exposure does not have to be a by-product of work to be tortious – it may also be deliberately created noise exposure.
Thus far, we are yet to see any ‘cataclysmic’ effects on ‘music making in the UK’, instigated by Goldscheider, but we will be able to make the same sweeping statement in 2021?
Tinnitus in RTA Claims
On account of the fact that small claims limit reforms, predominantly affecting road-traffic accident (RTA) claims, have been delayed by exactly 1-year, last year’s ‘Horizon Scan’ warning that motor insurers could see increasing numbers of (RTA) claimants also seeking compensation for otologic injury applies equally to 2021 – assuming there are no more delays.
In edition 293 (here), we analysed a plethora of epidemiological literature to gauge whether there is a biomechanical or biochemical link between conventional soft tissue injuries and tinnitus, but were unable to definitively state that they were unconnected.
Unfortunately, tinnitus adds an unwelcome dimension, complexity and costly element to RTA claims at a time when such claims were finally supposed to become more manageable.
EXHAUST FUMES
Diesel Exposure Mitigation Study (DEMiSt)
Diesel exhaust emissions (DEE) increase the risk of developing lung cancer [see the International Agency for Research on Cancer’s (IARC) Group 1 carcinogen classification, in 2012], chronic obstructive pulmonary disease (COPD), type-2 diabetes and infertility.
We also reported, in edition 316 (here), that metal nanoparticles in environmental air pollution (comprising of DEE) were responsible for a ‘silent epidemic’ of cardiovascular disease, before going on, in edition 317 (here), to report that air pollution had been associated with heightened incidence of Parkinson’s disease and dementias.
In last year’s ‘Horizon Scan’, we announced that the Institution of Occupational Safety and Health’s (IOSH) Diesel Exposure Mitigation Study (DEMiSt) had come to an end.
The ‘largest real-world in-vehicle personal exposure study to date’ was designed to investigate 141 professional drivers’ occupational exposure to DEE, or ‘black carbon’ (a proxy measure) over the course of almost 12,000 hours.
Later than expected, the full and final report was published, in July 2020.
This revealed that, on average, 18.6% of the professional drivers’ time was spent ‘at work driving’ and this accounted for 36.1% of their total black carbon exposure. Meanwhile, 54.4% of their time was spent ‘at home’, but this was only responsible for a 31.8% contribution towards their total black carbon exposure.
Moreover, drivers were exposed to 4-times more airborne black carbon [4.1 micrograms per cubic metre of air (µg/m3)] when ‘at work driving’ than when ‘at home’ (1.1 μg/m3). Taxi drivers were among the most exposed (6.5 µg/m3), closely followed by couriers (5.5 μg/m3), waste removal drivers (4.3 μg/m3), heavy freight drivers (3.9 μg/m3), utility service drivers (3.1 μg/m3) and emergency service drivers (2.8 μg/m3), while bus drivers were the least exposed (2.3 μg/m3).

[Source: Flickr – Garry Knight (30 September 2016): ‘Taxi Traffic’]
Drivers also experienced spikes of black carbon exposure, peaking at 100 µg/m3 and lasting up to 30-minutes, as fumes lingered in vehicle cabins. These peaks typically occurred in congested Central London traffic, car parks, depots, tunnels and ‘street canyons’ (between high buildings).
Lead researcher and Senior Lecturer at Imperial College, Dr. Ian Mudway, remarked that it was noticeable to see ‘just how surprised drivers taking part in the study were at the levels of their exposure to diesel’.
In 2021, we will be looking out for articles that promote the implementation of low-cost changes that were recommended by researchers as intermediate steps to reduce hazardous DEE exposures, which DEMiSt drew attention to:
- Always drive with windows closed.
- Use the recirculating ventilation function with vehicle windows closed, but only for short periods in high pollution areas.
- Carefully consider route choice to avoid areas of high congestion and try to avoid tunnels.
- Reduce driving frequency during peak evening hours (4 pm to 7 pm).
- Move shifts from weekdays to weekends.
- Rotate drivers if there is a risk of isolated workers being disproportionately exposed.
- Use in-cabin filters in certain circumstances.
We will also continue to inspect the work of Government in implementing British Safety Council (BSC) advice, compiled in its Time to Breathe White Paper, (2019), which advocated for:
- Health and Safety Executive (HSE) recognition of exposure to ambient air pollution as an occupational health issue and adopt a Workplace Exposure Limit (WEL) for Diesel Engine Exhaust Emissions (DEEE).
- Improvements for pollution monitoring across the UK, so that all regions have the same accuracy as London for emissions data.
- The UK’s adoption of World Health Organisation (WHO) exposure limits for the main pollutants of nitrogen dioxide, particulate matter and ozone:
- PM 2.5: less than 25 μg/m3 (24-hour mean) or 10 μg/m3 (1-year mean); and
- PM 10: less than 50 μg/m3 (24-hour mean) or 20 μg/m3 (1-year mean).
- A nationwide-reduced carbon footprint reduction.
RADIATION
UV Radiation
We alluded to future work of the Industrial Injuries Advisory Council (IIAC) in last year’s ‘Horizon Scan’ and we can now confirm that the investigation into the relationship between melanoma and airline crew exposure to ultraviolet (UV) radiation was conducted and findings published – the full report can be accessed here.
UV radiation from the sun is classified by the WHO as ‘carcinogenic to humans’ (Group 1 carcinogen).
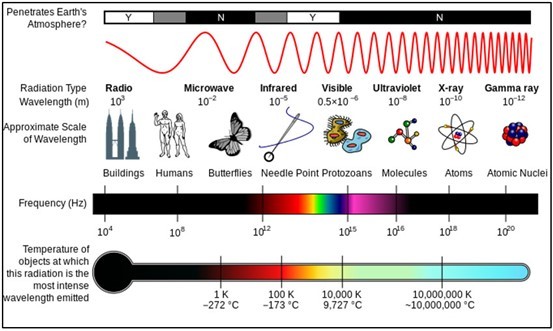
[Source: Wikimedia Commons – NASA (26 October 2007): ‘EM Spectrum’]
And now, the Council recommends that malignant melanoma in pilots and cabin crew should be added to the list of prescribed diseases (PD) for which benefit is payable, following ‘5-or-more-years aggregated duration of employment’.

It was convinced by ‘substantial and consistent evidence that there is more than double the risk of malignant melanoma in pilots and cabin crew and for pilots in particular, after 5,000 aggregated hours’ flying time’. This happens to correspond to approximately 5-or-more-years of aggregated duration of employment.[14]
The consequences of prescription on volumes of civil claims for the same will be on our radar in 2020. As will our interest in allegations that there is also an increased risk of melanoma in air traffic controllers, an area of research which the Council identified when completing its widescale literature review. Additionally, we will keep an eye on the evolving tendencies of employers to adopt sun safety policies for outdoor workers.
Mobile Phones and the 5G Era
In last year’s ‘Horizon Scan’, we previewed a class action lawsuit which was alleging that smartphones (including iPhone 7s, iPhone X, iPhone 8, iPhone 8 Plus, Galaxy S9, Galaxy S8 and Galaxy J3) were exposing users to levels of radiofrequency radiation (RFR) that ‘far exceed federal guidelines’.
In October 2020, however, it was disclosed that both Apple and Samsung had escaped legal proceedings and poured cold water over the Chicago Tribune investigation upon which these product liability claims were based.[15]
Mobile phones use non-ionising, ‘low power’ (low frequency) radio frequency electromagnetic radiation (RFR), emitted by in-built mobile phone antennae, in order to connect to networks wirelessly.
Although the latest 5th generation technology (5G) uses higher frequency RFR than its predecessors (reported here), it is still incapable of penetrating the body at a cellular level and therefore unlikely to cause cancer, as some people have alleged.
Tariff provider, EE, claims that RFR levels of 5G are within internationally agreed limits, specified by The International Commission on Non-Ionizing Radiation Protection (ICNIRP) Guidelines, but has previously been criticised for having stated, in 2017, that it could not provide ‘absolute assurance that research in the future won’t establish links between radio frequency emissions and health risks’.
In the space of the past year, though, the US FDA has reviewed the available epidemiological literature and assures that ‘there is no consistent or credible scientific evidence of health problems caused by the exposure to radio frequency energy emitted by [mobile] phones’.
Also in edition 312 (here), we gave an update on the progress of Imperial College London researchers’ involvement in the Cohort Study of Mobile Phone Use and Health (COSMOS), with preliminary findings demonstrating that those who use mobile phones extensively for making and/or receiving calls are reporting more frequent weekly headaches than other users.
However, the team considers that this is more likely to be associated with lifestyle factors than RFR emissions.
We will continue to monitor the science in the year ahead.
CONCUSSION AND SUB-CONCUSSIVE TRAUMA
We urge our readers to read our news article in this week’s edition to get up-to-speed with impending group litigation, advanced by ex-professional rugby players and ex-professional footballers with brain damage.
One could argue that of all of the ‘emerging risks’ to feature in last year’s ‘Horizon Scan’, this is the occupational health issue that has ‘emerged’ the most.
To-date, the academic literature in this field can be stratified into 1 of 4 groups:
- The long-term prevalence of neurodegeneration in footballers.
- The short-term effects of heading/sub-concussive impacts on cognition.
- The biomechanics of heading/sub-concussions.
- The influence of ball technologies (i.e. leather vs synthetic plastics) and styles of play on frequency and force of bodily impacts.
Most recently, researchers at the University of Leeds found that the speed of a football (up to 80mph in the modern professional game) in the air has more effect on impact damage than its weight or the material it is made from, thus denoting that modern footballers could be at even greater risk than those who played with older leather footballs:[16]
‘… the force experienced by the head during football heading is mainly influenced by the speed of the ball rather than its mass or stiffness’.[17]
Another recent study, conducted by Liverpool Hope University, exposed that the ‘working memory’ of a small sample of footballers declined by as much as 20% immediately after heading a ball 20 times.[18]
Elsewhere, data collected by Stats Perform, on behalf of the University of Glasgow, demonstrated that, at the highest level of global competition (World Cup tournaments), the number of headers-per-game has increased over time. World Cup matches from 1994 to 2018 averaged 93 headers-per-game, peaking at 105-per-game in 2002. Juxtapose this against an average of under 71 headers-per-game between 1966 and 1990, with a low of 59-per-game in 1970.[19] In short, footballers’ heading exposure has been on the rise.
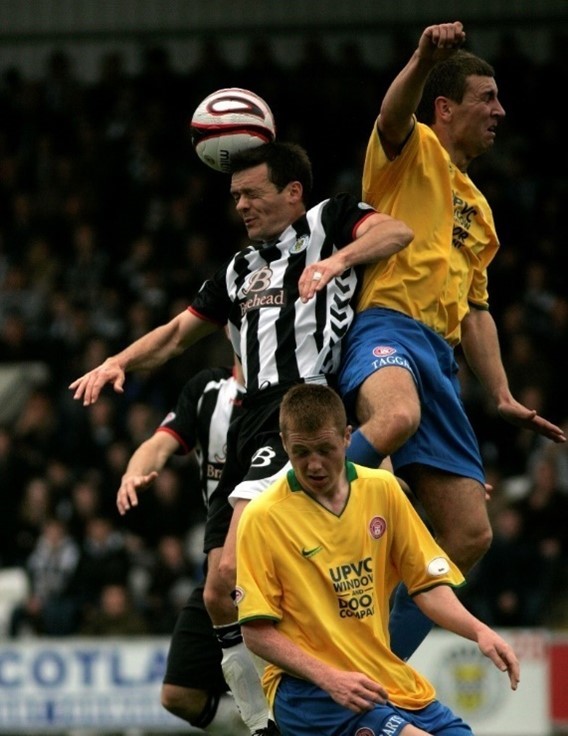
[Source: Wikimedia Commons – Alasdair Middleton (23 May 2009): ‘Header (St Mirren 0-1 Hamilton Academical May 2009’]
Plainly, however, none of these studies/study types are poised to say conclusively that long-term repeated heading of a football causes dementia, CTE or any other neurodegenerative condition. One cannot escape from the fact that any such claims are mere deductions, persuasive or not.
An advocate of this position is Dr. Vincent Gouttebarge, Chief Medical Officer at FIFPRO (the international players’ union), who cautioned against illegitimate rule changes in the absence of reason:
‘I know in the UK you have referred to the very good study [FIELD] from Professor Willie Stewart, but I looked at the study again this morning and I didn't see the words “heading” or “concussion” mentioned one time in this study.
Based on that study a lot of media in the UK made the conclusion that heading the ball or concussion lead to dementia, and I don't think this is a very thorough conclusion.
I don't think we have the scientific evidence with this study that there is a causal relationship between heading the ball, concussion and dementia’.[20]
The Football Association’s (FA) Medical Chief, Charlotte Cowie, has repeatedly concurred with this line of thinking.[21]
With the British Associated Press noticeably taking little interest in the ‘scientific method’, the past few months has seen a whirlwind of tabloid outbursts.
In October of this year, Alan Jarvis became the second ex-professional footballer, after Jeff Astle, to have his death (in December 2019, aged 76) formally recognised as an ‘industrial disease’ by a coroner in Ruthin. The inquest heard how he had once been knocked unconscious after a ball struck his face, forcing him to spend 2-weeks in hospital with a detached retina:[22]
‘The situation is by no means unequivocal. It must be very clear I am not saying playing professional football always causes dementia … but, on the balance of probabilities in Mr Jarvis' case, his previous occupational history has been a factor in his neuro generative functioning and had led to Alzheimer's disease’.[23]
Both Mr. Astle and Mr. Jarvis were diagnosed with CTE by leading expert neuropathologist, Dr. Wille Stewart.
In what felt like a perpetual stream of news, we then discovered that Nobby Stiles had died with Alzheimer’s and vascular dementia and almost instantaneously went on to discover that Sir Bobby Charlton had been diagnosed with dementia. These were the 4th and 5th members of England’s 1966 World Cup-winning squad to receive a dementia diagnosis, respectively, in the wake of Martin Peters, Ray Wilson and Jack Charlton.
Akin to the 1966 team, an investigation by Sky News Sport Correspondent, Martha Kelner, subsequently unearthed that more than half (6 out of 11) of the footballers who played for Burnley FC in their championship winning 1959/60 season have died from (or are suffering with) dementia.[24]
Dr. Stewart has, in recent days, confirmed post-mortem CTE in Mr. Stiles.[25]
As a consequence of high frequency media attention, a number of high-profile individuals in the sport have called for a complete ban on heading in training sessions at all levels of the game and for more research into the effects of heading on the brain.[26] Others have called for ‘aerial challenges’ to be classified as ‘dangerous play’,[27] while the Professional Footballers’ Association (PFA) has called for an ‘urgent intervention’ on heading.[28]
There has been an outpouring of former professionals who have now made their dementia diagnoses public[29] and pledged to donate their brains for science, after death.[30] It is believed that around 500 retired footballers have been affected, but a database is ‘desperately’ required to keep a record of this.[31]
What is more, Nike and Adidas have been called upon to create a ‘heading ball’, designed to minimise head impacts in training.[32]
On 16 November, The Daily Mail announced a new 7-Point Charter campaign, in conjunction with Alzheimer’s Society’s Sport United Against Dementia, insisting on:
- Increased funding from the FA and PFA for independent research into dementia and its links to football.
- The PFA to provide respite for families/carers of former professional footballers living with dementia.
- The PFA to appoint a dedicated ‘dementia team’ and work with, promote and financially assist Alzheimer’s Society’s Sport United Against Dementia (SUAD) campaign and Dementia Connect support line.
- The PFA to help fund regular social events for people living with dementia and their carers.
- Dementia to be formally recognised as an industrial disease.
- Football’s lawmakers, the International Football Association Board (IFAB), to immediately ratify temporary concussion replacements.
- Clubs to limit heading at all levels including professional (maximum of 20 headers-per-session in training and minimum 48-hours between sessions. [33]
How are governing organisations acquiescing to these demands?
Well, the PFA has already set up the Neurodegenerative Disease Working Group (NDWG), a task force with the specific purpose of examining the issue of brain injury diseases in football.[34] Moreover, IFAB has approved concussion substitutes, beginning in January 2021.[35]
As regards to ‘industrial disease’ prescription, we are aware that Dr. Stewart will not present his case before the IIAC until January 2021 at the earliest and a decision is unlikely before next summer.[36]
Pre-emptively, the Council has cautioned proponents that it will require more than just a ‘single study’ to recommend prescription. There must be ‘clear and consistent evidence across a number of studies’.[37]
Nevertheless, Dr. Michael Grey, the eminent neuroscientist at University of East Anglia (UEA), who is leading the SCORES project, considers IIDB designation to be ‘realistic … I think it's a case of “watch this space”’.
SCORES will explore the early signs of dementia in footballers (35 former professionals have already signed up and will be added to a pool of 40 amateurs and 60 control subjects, all over the age of 40[38]). We await news of study results, which will be published in BC Disease News in due course.
TEXTURED BREAST IMPLANTS
A year ago, we announced that Leigh Day Solicitors had issued letters of claim on behalf of claimants who were alleging that textured breast implant had caused them to develop a rare form of non-Hodgkin lymphoma, called anaplastic large cell lymphoma (ALCL), or breast implant-associated (BIA) ALCL.
BIA-ALCL was classified as a ‘disease’ by the World Health Organisation (WHO), in 2016, and 2-years later, cosmetics manufacturer, Allergan, removed its Biocell textured implants from European markets.
Contrary to presumption, however, the UK Medicines and Healthcare products Regulatory Authority (MHRA) subsequently stated, in regards to Allergan products, that:
‘There is currently no evidence of an increased risk to patients and there is no need for people who have Allergan breast implants to get them removed or have any additional clinical follow-up’.
As at 15 December 2020, there were 992 recorded cases of BIA-ALCL worldwide, which translates to almost double the figure disclosed last year (650).[39]
Nevertheless, the MHRA’s position has not budged and litigation has not received substantial press this year, except to divulge that High Court proceedings had been issued by 65-year old, Susan Axelby, in March 2020 – read our article in edition 307 (here).
Further, that Ms. Axelby’s product liability case has been advanced under Part 1 of the Consumer Protection Act 1987 and will assert that the product used was ‘defective’ i.e. that the ‘safety’ of her implants was ‘not such as persons generally are entitled to expect’. She would not have accepted them, had she known that there was a direct risk of ‘death or personal injury’ (see s.3 of the Act).
Perhaps the coming year will shed more light on this emerging health risk?
RESPIRABLE CRYSTALLINE SILICA: ‘THE NEXT ASBESTOS’
Ensuing last year’s ‘Horizon Scan’, in which we previewed the All-Party Parliamentary Group (APPG) for Respiratory Health’s extensive inquiry into the disease burden of silicosis on the construction industry, we were alarmed, earlier this year (here), to read that the APPG had dubbed respirable crystalline silica (RCS) ‘the next asbestos’ – to access the full report, click here.
RCS is created when silica-containing materials are ‘fractured’, i.e. cut, drilled into, or polished. These materials include:
- Sandstone, gritstone and quartzite (more than 70% silica);
- Concrete and mortar (25-70% silica);
- Shale (40-60% silica);
- China stone (up to 50% silica)
- Slate (up to 40% silica);
- Brick (up to 30% silica);
- Granite (up to 30% silica);
- Ironstone (up to 15% silica);
- Basalt and dolerite (up to 5% silica); and
- Limestone, marble and chalk (up to 2% silica).
RCS exposure can lead to irreversible and often fatal silicosis, which is the most common occupational lung disease worldwide and considered an ‘emerging occupational health epidemic’. It is also linked with tuberculosis, kidney disease, arthritis, chronic obstructive pulmonary disease (COPD), lung cancer and chronic bronchitis.
In spite of this, research has unearthed that there is a ‘profound lack of awareness among construction workers about the risk of RCS exposure’ – a workforce which constitutes 81% of an estimated 600,000 British workers exposed on an annual basis [where the remaining 19% includes kitchen worktop fitters, textile (denim) machine operators and other professionals].
By starting a ‘long-overdue’ conversation about how to tackle the adverse and ‘under-documented’ health risks among affected workers, it appears that the APPG has now ‘recognised the urgency of the issue’.
Facing pressure from the British Occupational Hygiene Society (BOHS), in the year ahead, we intend to monitor the Government’s efforts to make good on several recommendations that emerged from the Report, namely:
- To make silicosis a reportable condition for those who are currently in work and exposed to RCS, under The Reporting of Injuries, Diseases, and Dangerous Occurrences Regulations (RIDDOR) 2013.
- To amend The Health Protection (Notification) Regulations 2010 to make silicosis notifiable through Public Health England, thereby creating a compulsory national silicosis register – in edition 283 (here), we reported that Unite and Thompsons Solicitors had created their own silica dust register.
- To develop and implement a targeted industry awareness campaign for those at risk of developing silicosis.
- To allow workers to hold their own occupational health records to encourage workers to make associations between symptoms and exposures.
- To merge occupational health services into GP surgeries to allow for occupational histories to be accounted for where work-related ill health is suspected.
- To introduce new Governmental health and safety regulations [outside of the Control of Substances Hazardous to Health Regulations 2002 (COSHH)] specifically relating to the control of respirable crystalline silica (RCS), so that it is afforded the same level of protection as asbestos.
- To investigate (through the NHS) a screening programme for those exposed to RCS.
- To provide access to occupational health services for RCS-generating industries.
- To halve the workplace exposure limit (WEL) for RCS in the UK from 0.1mg/m3 to 0.05mg/m3 (see the 4th edition of EH40/2005), in line with the 2003 recommended exposure standard from the Scientific Committee on Occupation Exposure Limits (SCOEL), and ensure that statutory monitoring requirements are in place to reduce over-exposure.
- To implement Health and Safety Executive (HSE) requirements, compelling compulsory use of masks, dust extraction and water suppression, along with annual reporting of inspection and compliance levels.
- To increase HSE resources to raise the volume of on-site inspections of building contractors of all sizes.
BOHS estimates that every year, there are approximately 500 UK construction workers deaths from silicosis and approximately 4,000 deaths from chronic obstructive pulmonary disease (COPD), all attributed to RCS exposure.
PART 2 – COVID-19 INFECTION CLAIMS
WHAT IS COVID-19?
The virus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the resulting disease, COVID-19, has gripped the world in 2020.
Those infected, who present with symptoms, typical complain of a high temperature, a new, continuous cough and/or a noticeable loss or change to their sense of smell or taste.[40] However, skin rashes,[41] hearing loss,[42] muscle aches and pains, fatigue and gastrointestinal symptoms have also been recorded among COVID-19 sufferers.[43]
For some (including the elderly, smokers, pregnant women, members of the BAME community, those with comorbidities, those who are immunocompromised, etc.), these mild symptoms can become more serious, as the virus proceeds to the next phase – attacking the lungs. This can lead to severe pneumonia with breathing difficulties, or even respiratory failure [acute respiratory distress syndrome (ARDS)].[44] In some cases, these adverse effects can be fatal. Over the past year, clinicians have also found that COVID-19 can cause ‘extrapulmonary manifestations’, i.e. sickness beyond the lungs.[45]
Whilst there is growing evidence to suggest that infections occur by way of airborne exposure to the virus [where viral particulates are less than 5 micrometres (µm) in diameter],[46] established science has only confirmed thus far that the spread of disease occurs via droplet transmission.
For instance, if an uninfected bystander stands in close contact with an infected person (‘within 6 feet of an infected person for a cumulative total of 15 minutes or more over a 24-hour period’[47]) and inhales the respiratory droplets produced when an infected person coughs, sneezes, talks or breathes.[48]
Alternatively, droplet transmission can arise if uninfected person touches a contaminated surface, or the hand of an infected person, before going on to touch their own mouth, nose or eyes.
TO WHAT EXTENT HAS COVID-19 AFFECTED THE UK PUBLIC?
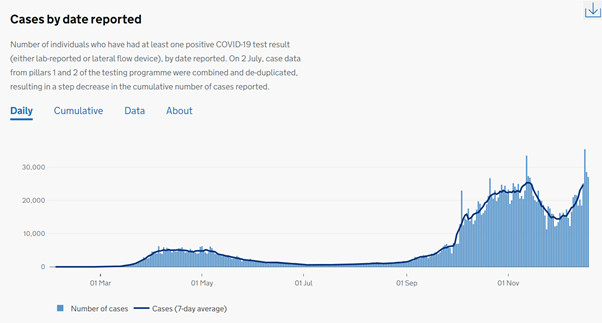
As at 19 December 2020, a total of 2,004,219 people had tested positive for COVID-19, in the UK.[49]
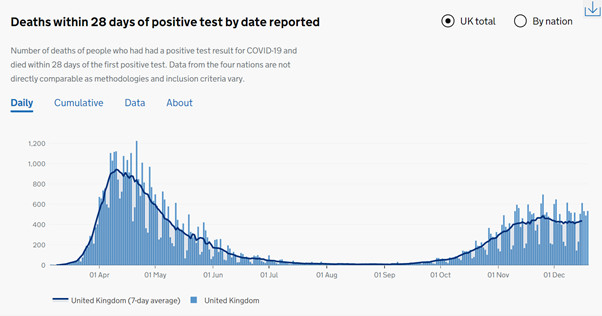
Moreover, up to 19 December 2020, a total of 67,075 people had died within 28 days of a positive COVID-19 test result, while up to 4 December 2020, a total of 76,287 people had died with COVID-19 listed on their death certificate.[50] The former metric of mortality is the work of the Department of Health and Social Care (DHSC), while the latter is the work of the Office for National Statistics (ONS).[51]
Are cumulative case numbers and deaths set to continue rising?
We are currently in the 2nd wave of COVID-19 (also described as the 2nd phase of the 1st wave) and incidence of the disease is growing. On 18 December 2020, the rate of infection, or ‘R number’, was estimated to be between 1.1 and 1.2 for the whole of the England (with lows of 0.9 in the North and highs of 1.4 in the East).[52] Mathematically speaking, this means that, for every 1 person exposed, between 1.1 and 1.2 people will be infected.
The mortality rate, meanwhile, was most recently analysed by Imperial College London.[53] Researchers investigated fatalities in high income countries by screening 175 studies and identifying 10 representative antibody surveys. They concluded that 1.15% of people who are infected with COVID-19 go on to die and that the risk of death increases with age:
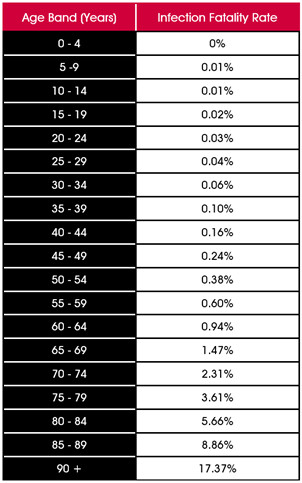
For those who have been infected, experts have remarked that the risk of being infected again is low, given that 6-months into the pandemic, there had only been 4 or 5 cases of confirmed reinfection across the entirety of Europe.[54]
However, journal articles have also chronicled that antibody levels in those who have produced a natural immune response to the virus have declined rapidly within a few weeks/months of infection (unlike SARS-CoV-1 antibodies, which lasted around 3-years before dwindling).[55]
The silver bullet to COVID-19 deaths is, of course, a 100% effective vaccine, which stimulates an immune response targeted to fight the virus and could potentially bring about herd immunity.
On 2 December 2020, the Medicines and Healthcare products Regulatory Agency (MHRA) approved the first COVID-19 vaccine,[56] which was developed and trialed by Pfizer/BioNTech and is supposedly 95% effective.[57] By 16 December 2020, 137,000 people had been inoculated in a series of 800,000 scheduled doses. This included people over the age of 80, care home workers and NHS staff.[58]
The next serum to receive MHRA approval is likely to be the Oxford University/AstraZeneca vaccine, possibly in the week commencing 28 December 2020.[59] This is 1 of 15 vaccines to undergo large-scale Phase 3 efficacy trials, with more than 170 teams of researchers worldwide having entered the race to develop a COVID-19 vaccine.[60]
In recent days, a new strain of SARS-CoV-2 has been identified in England and the World Health Organisation (WHO) has been warned about this novel variant, which appears to be up to 70% more transmissible, but less deadly.[61]
It is natural for viruses to mutate as they replicate, but it is not yet known whether the genomic changes recently seen in strands of SARS-CoV-2 will impair the success of vaccines and increase the long-term persistence of the virus.[62]
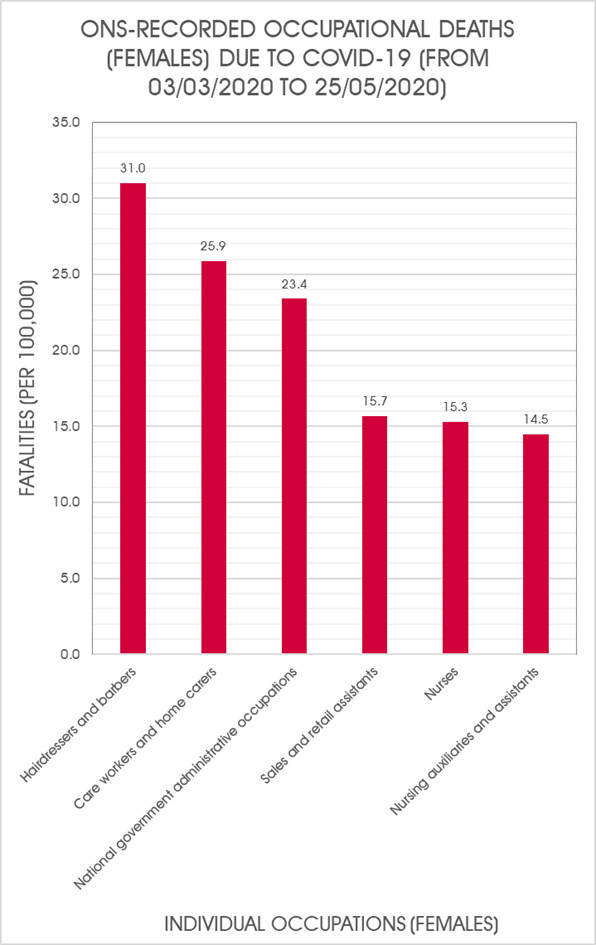
Back in June of 2020, the ONS revealed that 4,761 ‘deaths involving COVID-19’ in the ‘working age population’ had been registered in England and Wales between 9 March and 25 May 2020.[63] No updated occupational mortality data for this geographical region has been published by the ONS since.
Although 75% of jobs that require frequent contact with people are undertaken by females, male workers had almost double the risk of dying from the virus (19.1 deaths per 100,000 people) than their female counterparts (9.7 deaths per 100,000 people).[64] The ONS’s provisional mortality rates equated to 3,122 male deaths and 1,639 female deaths.
Below, we present bar charts to illustrate COVID-19 mortality (per 100,000) among workers of both sexes, separated by individual occupation [with reference to the 10th edition of the International Classification of Diseases (IDC-10)].
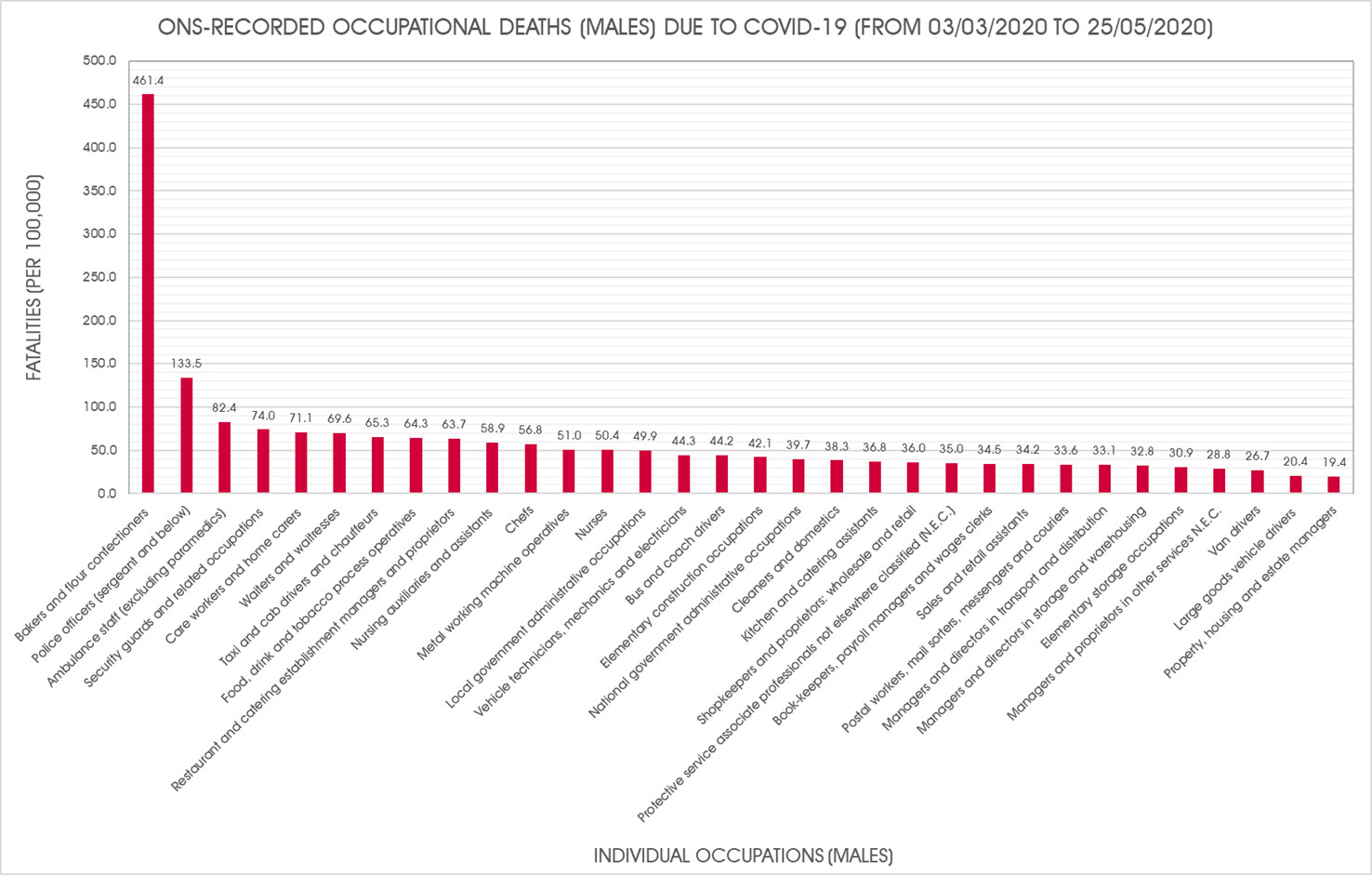
It has been well publicised that those most at risk of COVID-19 infection outbreaks have been ‘key workers’ and those unable to work from home. For instance, NHS staff and care home workers,[65] public transport workers,[66] food delivery drivers,[67] postal courier service workers[68] and essential retail / factory workers.[69]
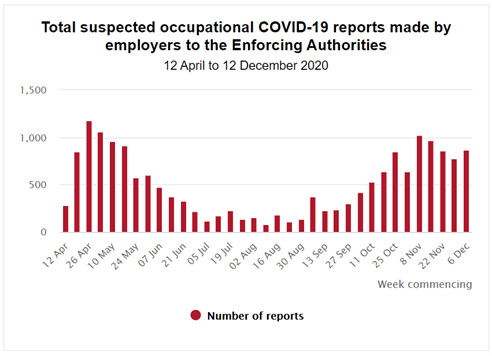
Another indicator of work-related SARS-CoV-2 infections is data collated under The Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013, by which employers are duty bound to report cases of, or deaths from, COVID-19, which related to occupational exposures.[70]
The latest published figures show that between 10 April 2020 and 12 December 2020, there were 17,895 notifications of occupational COID-19 in workers, including 223 deaths. Around half of the notifications received were made after September, as the ‘2nd wave’ of infections began to spike.[71]
EVIDENCE OF COVID-19 EMPLOYERS’ LIABILITY CLAIMS INFRASTRUCTURE?
The Law Society Gazette reported, in August, that ‘claims management companies haven’t tried to make money from coronavirus yet’. The Financial Conduct Authority has been preparing for an ‘epidemic of pandemic claims’ by allocating ‘extra resources to a potential surge in applications from [claims management companies] CMCs entering the Covid claims market’.[72]
Several newly incorporated entities with ‘CORONA’ or ‘COVID’ in the name began to appear on Companies House and these could foreseeably emerge as CMCs:

There may be some delay before CMCs become fully operational, but we will continue to survey the claims environment with interest in 2021.
As at 20 November, Litigation Futures revealed that around 30 compensation claims for COVID-19 infection had been registered with the Compensation Recovery Unit (CRU) – an early sign of increasing claims farming activity attracting both men and women disproportionately in the 50-59 age category. Thompsons has emerged as the dominant claims handling firm, with strong ties to trade unions.[73]
Another trend to look out in the coming months will be fraudulent claims (likely motor insurance claims) where COVID-19 is used as the ultimate ‘get out of jail free’ card to excuse inadequacies in the chronology of factual evidence, e.g. ‘COVID-19 symptoms’ prevented the victim from seeing their GP about ‘whiplash symptoms’ shortly after ‘accident’?[74]
COVID-19 INFECTION NEGLIGENCE CLAIMS
Should there be widescale COVID-19 infection litigation brought against employers next year, the issues that will be up for discussion will include:
- Whether adequate PPE has been supplied;
- Whether instructions to return to work have been delivered prematurely; and
- Whether work environments are generally safe.
Statutory Breaches?
Section 69 of the Enterprise and Regulatory Reform Act (ERRA) 2013 ultimately removed any claim for statutory breach of duty in a civil claim, whose origin stemmed from the ‘six-pack regulations’[75] (technically seven-pack) by repealing s.47(2) of the Health and Safety at Work Act (HSWA) 1974.[76]
Thus, in cases where breach of duty is alleged to have occurred after 1 October 2013, the claim must be brought under principles of common law negligence:
- Was the injury a foreseeable consequence of the claimant’s work?
- Did the defendant breach the common law standard of care owed to the claimant?
However, when answering the 2nd question, on what level of care is expected of an employer, courts have consistently found that a ‘reasonable’ employer should be aware of the historic Regulations and the duties that they imposed on employers.
In practice, therefore, it is customarily assumed that s.69 of the 2013 Act has done nothing to substantially modify the employer’s duty of care, other than to reverse the burden of proof from the defendant to the claimant – see Gilchrist v Asda [2015] CSOH 77 – though COVID-19 infection cases may ‘test’ this assumption. Courts may be ‘far more prepared than usual’ to ‘look beyond’ the ‘strict language’ in the Regulations and ‘seriously’ consider arguments relating to ‘reasonable practicability’.
If Regulations are considered relevant to breach of duty arguments in COVID-19 infection claims, several duties owed by employers under the PPE Regulations 1992 could be placed under the microscope:
- REGULATION 4 – Ensuring the provision of suitable PPE (i.e. appropriate and fits well).
- ‘… except where and to the extent that such risk has been adequately controlled by other means which are equally or more effective’ – a ‘last resort’?
- REGULATION 6 – Ensuring that risk assessments are conducted.
- As ‘a reasonably prudent employer’ would (Threlfall v Kingston-upon-Hull City Council [2010] EWCA Civ 1147)
- REGULATION 7 – Ensuring the maintenance and replacement of PPE.
- REGULATION 9 – Ensuring that information, instruction and training on use of PPE is given.
Where elements of the PPE Regulations, for instance, are cited, one might presume that the following questions could be asked:
Advice has changed drastically over time, in line with changing scientific opinion and technological advancement.
- At the time of the alleged breach, what was the Government/WHO/PHE/HSE guidance regarding the effectiveness of certain PPE?
- At the time of the alleged breach, should risk assessments have been re-done if there was a ‘significant change’ to the basis of the risk assessment, e.g. when members of the BAME community were found to be at disproportionate risk of COVID-19 outcomes?
Supply and demand chains have been stretched throughout the pandemic, affecting the accessibility, quality and cost of PPE.
- At the time of the alleged breach, was authentic PPE readily available and at what price (versus the means of the employer)?
- Was there enough PPE to prevent reuse, where such practice was ill advised by the British Standards Institute (BSI) and others?
The pandemic caused businesses to adapt to survive.
- At the time of the alleged breach, what were market competitors simultaneously doing?
Some workers, (e.g. supermarket workers, bus drivers) may have never used PPE in their working lives before COVID-19.
- Was action taken by the employer to ensure that enforced PPE would be properly donned, effective against infection and also comfortable?
Common Law Duty of Care
In light of s.69 of the ERRA, it is of course important to also consider the default common law duty of care in situations where there is fast-developing knowledge.
In occupational disease claims, the courts have commonly applied the test set out in Stokes v Guest Keen and Nettlefold (Bolts and Nuts) Ltd [1968] 1 WLR 1776, which established the ‘reasonable and prudent employer’ standard of care, whereby the employer may avoid liability in negligence if it takes precautionary action based on ‘what he knows or ought to know’ and keeps ‘reasonably abreast’ of developing knowledge and is ‘not … too slow to apply it’.
Stokes was also cited and followed by Simon J, in Asmussen v Filtrona United Kingdom Ltd [2011] EWHC 1734 (QB):
‘… the foreseeability of injury is to be tested against the standard of the well-informed employer who keeps abreast of the developing knowledge and applies his understanding without delay, and not by the standard of omniscient hindsight. An employer can rely upon a recognised and established practice to exonerate itself from liability in negligence for failing to take precautionary steps unless (a) the practice is clearly bad practice, or (b) in the light of developing knowledge about the risks involved in some location or operation, a particular employer acquired greater than average knowledge of the risks’.
By its own admission, the Government has elevated itself to a position of inspiring ‘confidence’ in providing the ‘most up-to-date’ and ‘transparent’ science advice, based on information supplied by the Scientific Advisory Group for Emergencies (SAGE):
We have … published the statements and the accompanying evidence to demonstrate how our understanding of COVID-19 has continued to evolve as new data emerges, and how SAGE’s advice has quickly adapted to new findings that reflect a changing situation’.[77]
Thus, it is essential in any COVID-19 infection claim that the employer’s duty of care is considered against what is known at the time of exposure, with specific reference to Governmental, industry and scientific knowledge of the time and disapplying later knowledge and hindsight. Ordinarily, they will not be burdened with special, earlier knowledge, or be held to a more onerous standard of care.
What reference point should be taken for the consideration of the ‘established practice at the time’? This is likely to be the state of knowledge and guidance as existed shortly before and during a claimant’s incubation period – up to 14 days from exposure / infection to the development of symptoms.
Thus far, the Government has, among a host of measures, intermittently introduced lockdowns and the 4-tier system; social distancing and grouping rules; restrictions to business opening hours and forced business closures; mandatory face coverings; air corridors; and various means of testing and tracing COVID-19 incidence and viral transmission. It has also produced various pieces of industry-specific practical guidance documents:
- Work in construction and other outdoor work;
- Work in factories, plants and warehouses;
- Work in laboratories and research facilities;
- Work in other people’s homes;
- Work in offices and contact centres;
- Work in restaurants, pubs, bars and takeaway services;
- Work in shops and branches;
- Work in or from a vehicle;
- Work in close contact services;
- Work in hotels and other guest accommodation;
- Work in heritage locations;
- Work in the visitor economy;
- Work in the performing arts; and
- Work for providers of grassroots sport and gym/leisure facilities
In kind, employers have enforced a host of protective procedures, including the mandatory wearing of surgical masks, respirators, spit hoods, plastic visors and gloves; the undertaking of COVID-19 risk assessments, checks on mental and physical wellbeing and record keeping of all staff and contractors on site; the installation of Perspex shields, protective screens; paperless filling systems and air filtration / purification units; the making available of antibacterial hand gels; the use of ultraviolet light sanitisers, robot cleaners and temperature screening equipment; the setting-up of one-way systems, enhanced cleaning regimes (handwashing and surfaces), separated workstations (for social distancing purposes) and limited person quotas in given locations; and the turning away of potentially infected staff.

[Source: Geograph – Jaggery (6 April 2020): ‘Let's keep a safe distance - Please follow the one-way system, Tesco Express, Malpas, Newport’]
Contesting Breach of Duty
Contributory Negligence?
Failure on the part of an employee to follow proper social distancing, wash hands properly and on a regular basis, or adopt other required precautions, will likely work in a defendant’s favour when defending claims.
The Doctrine of Volenti Non Fit Injuria?
Many retirees have sought, albeit unselfishly, to return to the world of work and volunteer, in a time of crisis. If a person has comorbidities and is knowingly exposing themselves to the risk of adverse COVID-19 health consequences, have they consented to their employer’s negligence and does the defendant have a complete defence to the claim? Volenti is a rare defence, not least because it is unpopular for courts to reach such a finding (that a claimant has acquiesced to negligence). In certain circumstances, however, volenti may be a valid defence – and this may be one such circumstance.
Acting on Necessity?
If a defendant supermarket, for example, found itself unable to comply with its duty to keep employees safe in the midst of an outbreak, could it submit that its decision to continue regardless and not close operations was legitimised by its contribution to the ‘national effort’?
Waiting for Complete Guidance?
If a claimant were to propose that their employer failed to reassess risk in line with new science, defendants may seek to cite the military Q fever case of Bass v MOD [2020] EWHC 36 (QB), in which the High Court accepted that, whilst employers must be alert to changing evidence, they are entitled to take a cautious approach and wait for more complete evidence before undertaking a new risk assessment.
Defendant businesses may, to some extent, be absolved by the slow and incoherent action of the Government to define a clear and exhaustive strategy on COVID-19 prevention. As Professor Andrew Watterson, of the University of Stirling, rationalised in a New Solutions journal article:
‘In due course, there will need to be a thorough analysis of the national and regional performance of the UK and devolved governments during the pandemic, why some decisions and actions varied between them and with what effect on employee health and safety across society. Also the wisdom of the devolved administrations accepting initial UK government policy and agency assessments of pandemic risks should be scrutinized. The first UK timetable for actions rather than those of the WHO with its extensive evidence-based reports on pandemics was seriously flawed. The implications for occupational health and safety were considerable’.[78]
The Duty to Dismiss Vulnerable Employees?
If a worker is particularly susceptible to COVID-19, questions may be asked of an employer’s duty to balance ‘freedom of the individual’ against the responsibility to ensure that their employee is safe.
The guiding authority on this issue is still the occupational dermatitis case of Withers v Perry Chain Co Ltd [1961] EWCA Civ 4, which found that there is no common law duty ‘requiring an employer to dismiss an employee rather than retain him or her in employment and allowing him or her to earn wages, because there may be some risk [of harm]’. On the contrary, it is generally for the employee to decide whether or not to take the risk, weighing that risk ‘against the desirability, or perhaps the necessity, of employment’. That being said, Withers does not always apply and is a matter for assessment on a case-by-case basis.
In the case of Coxall v Goodyear Great Britain Ltd [2002] EWCA Civ 1010, the Court of Appeal clarified, for the first time, that the ‘principal consideration in determining whether or not any particular case falls within the Withers principle’ is the ‘magnitude of the risk’ of injury, i.e. ‘the actual nature and extent of the known risk’.
However, an important obiter observation recognised that, were a claimant to ‘insist’ that they ‘wish to go on working’ after discussing all the available options with their employer, prospects of repudiating the claim would vastly improve.
Medical & Legal Causation
Medical Causation
We assume that proving medical causality between exposure within the workplace/public spaces and infection will be a more challenging hurdle to surpass than proving breach and this discrepancy was exacerbated in the early stages of the pandemic when testing and tracing capabilities were limited. That being said, determining exactly where (location), when (time) and how (source) an alleged tortious exposure took place is still an imperfect science.
Investigating medical causation will require a detailed forensic review of the likely incubation period, working back up to 14-days prior to the first onset of symptoms. What was a person’s activity during this period and what were all the potential periods, durations, frequencies and types and doses of exposure?
Legal Causation
Deciding which of the 4 legal causation tests (the ‘but for’ test / the ‘doubling of risk’ test / the ‘material contribution’ test / the ‘Fairchild v Glenhaven Funeral Services [2002] UKHL 22’ principle) applies to the facts of a specific occupational disease claim appears to depend on whether:
- There is a single cause of disease or multiple causes of disease.
- There is a single exposure source or multiple exposure sources.
- Where there are multiple causes, whether they act independently or together to cause disease.
- The scientific knowledge surrounding the aetiology of disease is well known or poorly understood.
- The disease is divisible or indivisible.
- The disease in question is mesothelioma.
Where there is a single cause of disease and a single exposure to the same, the ‘but for’ test is readily applied. However, the courts have had difficulty, in recent years, in applying the correct test of causation where (i) there are multiple sources of exposures to one known cause of disease, or (ii) there are multiple exposures to multiple causes of disease, or (iii) scientific and medical knowledge of aetiology of the disease is simply not sufficiently developed to say precisely how a disease has developed, or how potential multiple causes of the same may have contributed either to the disease itself, or to the risk of developing the disease.
In Zurich Insurance PLC UK Branch v International Energy Group Ltd (Rev 2) [2015] UKSC 33, Supreme Court Justices assented to the prospect of the Fairchild exception (causation met by proving that breach merely contributes towards the risk of injury, i.e. beyond de minimis exposure) applying ‘to any disease which has the unusual features of mesothelioma’, i.e. indivisible diseases (almost) exclusively linked to a single known type of exposure.
At the present moment in time, we cannot say with confidence that COVID-19 is a divisible disease, as the medical science on a viral dose-response relationship is still in its infancy.
Willem van Schaik, Professor of Microbiology and Infection at the University of Birmingham, predicts that the ‘infectious dose’ of SARS-CoV-2 is ‘in the region of a few hundred or thousand particles’. Similarly, Virology specialist at Imperial College London, Dr. Michael Skinner, tentatively considers that the ‘infectious dose’ is ‘around a hundred virus particles’ and being exposed to multiple infected sources is unlikely to make much difference to the course of disease, nor the outcome.
Owing to the fact that viruses reproduce exponentially, there may be no discernible dose-response relationship, but a 2015 study previously demonstrated that influenza did exhibit such a relationship, i.e. with higher viral dosages, the symptoms experienced worsened.[79] MERS and SARS also follow this pattern.[80] Veterinary Surgeon and Clinical Research Fellow in Viral Immunology at the University of Cambridge, Sarah Caddy, explains that this makes logical sense, as ‘the more starting virus particles there are, the more cells will be infected’.[81]
Needless to say, if the Fairchild principle does apply to COVID-19 infection claims, it would invariably lower the legal causation threshold.
Damages
Envisaging the probable value of EL/PL COVID-19 infection claims, in terms of general damages, we presume that the anecdotal sections of the Judicial College (JC) Guidelines (15th edition) would be:
- For a collapsed lung (£1,880 to £4,540) – Chapter 6(A)(f);
- For toxic fume/smoke inhalation (£4,540 to £10,750) – Chapter 6(A)(e); and
- For permanent breathing difficulties short of permanent breathlessness (£26,710 to £46,780) would be of relevance – Chapter 6(A)(c).[82]
As such, a claimant who was admitted to ICU with COVID-19 and survived would likely seek general damages in the £26,710 to £46,780 bracket, while a claimant who is admitted to hospital with COVID-19, but not transferred to the ICU, would warrant an award between £12,000 to £36,000.
Of course, claimants may also seek special damages for lost earnings and potentially future care (especially if there are long-term consequences of the virus). Depending on the findings of studies into long-term impacts of COVID-19, claimants may also seek compensation for other physical and mental damage caused by infection, which would be assessed in line with other JC Guideline brackets.
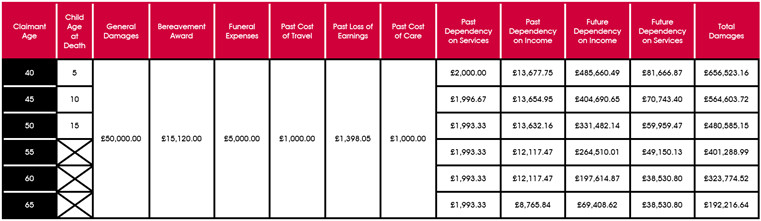
Example basic COVID-19 infection claim:
- A male care worker (aged 40/45/50/55/60/65) is on shift in a home where there is a COVID-19 outbreak.
- Due to his employer’s negligence, he contracts COVID-19.
- He is forced to take time off sick for 4-weeks, losing out on a proportion of his yearly salary [£18,237 per annum = Annual Survey of Hours and Earnings (ASHE) average for ‘Care workers and home carers’ (CODE 6145)].
- His symptoms are severe and he consequently dies, in May 2020.
- Had he not contracted the disease, he would life expectancy would not have been shortened and from the age of 65 through retirement, he would have received a £10,000 pension.
- He leaves behind his wife (and a temporarily dependent child), who has no personal income and an ordinary life expectancy.
- She has a £2,000 annual dependence on his services, up to the age 80.
- The deceased’s estate brings a claim against his former employer, producing a schedule of loss, comprising of general and special damages.
- The trial goes ahead 1-year after the date of death.
COMPLEX COVID-19 INFECTION CLAIMS
As time has gone by, the science has suggested that SARS-CoV-2 is not just a respiratory virus, but a ‘multi-organ killer’.[83]
There is a growing list of academic journal articles which link COVID-19 infection with a wide range of acute and serious health conditions, which include but are not limited to:
- Encephalitis, psychosis/delirium, dementia, Alzheimer’s, Parkinson’s and other types of brain damage (prevalence of around 50% of patients with severe COVID-19 infection[84]).[85]
- Tinnitus – an Anglia Ruskin University study of 3,103 people with tinnitus from 48 countries (the vast majority coming from the UK and the US) has found that that 40% of participants displaying symptoms of COVID-19 simultaneously experienced a worsening of their tinnitus.[86]
- Large vessel stroke (particularly in young patients) – blood tests show that COVID-19 infection makes the blood very sticky, i.e. more prone to clot[87] – ischemic stroke risk is 8-times greater than in influenza patients[88].[89]
- Other types of blood clot (9-times as many in COVID-19 patients as in swine flu patients[90]), e.g. deep vein thrombosis and pulmonary embolism[91].[92]
- Heart arrhythmia, congestive heart failure, myocarditis, pericarditis and other cardiovascular conditions (a global study of 1,261 COVID-19 patients found that 55% produced abnormal echocardiograms affecting the left and right chambers of the heart equally, even though 71% had never before been diagnosed with heart problems[93]).[94]
- Thrombocytopenia.[95]
- Sepsis (as many as 1 in 5 hospitalised COVID-19 patients, according to the UK Sepsis Trust).[96]
- Potentially ‘irreversible’ lung scarring (referred to as ‘ground-glass opacities’ in the literature[97]) affecting thousands (seen in 20 to 30% of patients, some of whom are asymptomatic).[98]
- Liver damage.[99]
- Gastrointestinal infection.[100]
- Sub-acute (De Quervain's) thyroiditis.[101]
- Acute and severe kidney injury (supposedly in up to 30% of patients[102]).[103]
- Diabetes (where the virus appears to damage the cells responsible for producing insulin[104]), including new-onset type 1 diabetes in children.[105]
- Cancer (with academics stressing that asymptomatic COVID-19 patients are at risk).[106]
- Testicular damage[107] and male infertility.[108]
- A type of temporary hair loss, called telogen effluvium, which typically occurs post-shock or after traumatic event.[109]
- Rare inflammatory multisystem syndrome (Kawasaki disease) in children[110] (especially in BAME patients and even more markedly so in those with African heritage[111]), which has been fatal for at least 2 British children[112] and is caused by ‘significant changes in white blood cells’.[113]
- COVID-19 in newborn babies (transmitted by the mother in the womb), though the benefits and safety of an infected mother breastfeeding outweigh any risk, says the WHO and the Royal College of Obstetricians and Gynecologists.[114]
- Vulnerabilities in the development of human embryos in the womb (with issues commencing as early as the 2nd week of pregnancy) – University College London has devised a study to quell fear of increased miscarriages and less successful pre-term labour deliveries.[115] [116]
More and more information is also surfacing on a common grouping of debilitating longer-term health complications faced by a ‘significant minority’ of COVID-19-infected patients,[117] which has been dubbed ‘post-COVID syndrome’ (or ‘long-COVID’).
‘An illness in its own right’,[118] sufferers have endured fatigue, breathlessness, fever, blurred vision, difficulty concentrating, memory loss (‘brain fog’) and heart inflammation – this is evocative of post-viral fatigue syndrome.
According to the latest King’s College research, published in October (based on data compiled by the COVID-19 Symptom Study App, designed by ZOE, the health science company), 1 in 20 infected COVID-19 sufferers have gone on to suffer symptoms lasting longer than 8-weeks.[119]
To ascertain the full extent of the long-term health effects of COVID-19, the £8.4 million Post-hospitalisation COVID-19 study (PHOSP-COVID) has been devised and was officially launched on 7 August.[120] The National Institute for Health Research (NHR) Leicester Biomedical Research Centre (BRC)-led project is recruiting 10,000 patients hospitalised with COVID-19 and will monitor post-symptomatic progression for up to 25-years.[121]
In July, the UK Government also launched ‘Your COVID Recovery’, an online portal for people in England to track symptomatic progress.[122]
ASYMPTOMATIC COVID-19 INFECTION CLAIMS?
As COVID-19 infection claims emerge and develop, it is inevitable that claims handling firms will look to convert what potentially could be a huge pool of asymptomatic individuals into negligence claims. Their success will surely depend on what evidence comes to light in respect of the long-term clinical sequelae of infection in the asymptomatic population.
Large numbers of COVID-19 infections have not translated with signs or symptoms of the virus and widescale antibody tests have already helped to confirm this – a University College London study of over 36,000 people living in Northern Ireland, England, and Wales found that as many as 86% were asymptomatic – the largest proportion to-date.[123]
Somewhat of a matter for future ‘concern’, therefore, is the growing body of research which has concluded that COVID-19 patients with mild-to-moderate symptoms, and even asymptomatic patients, are displaying signs of delayed onset health conditions, including lung scarring, thrombocytosis, stroke, cancer and brain damage – ‘hidden epidemics’.[124]
As a result, prospective COVID-19 infection litigation may involve complex discussion on principles of ‘actionable damage’ and de minimis non curat lex, as claimants, who have not yet suffered measurable pain, suffering or loss of amenity, seek compensation.
The question of what constitutes ‘actionable damage’ has been litigated before the courts in many disease claim types, such as pneumoconiosis (Cartledge v E Jopling & Sons Ltd [125]), asbestos-related pleural plaques (Rothwell v Chemical & Insulating Co Ltd[126]), asbestosis (Carder v The University of Exeter[127]), NIHL (Ross v Lyjon[128]) and most recently, platinum salt sensitivity (Dryden & Ors v Johnson Matthey Plc[129]).
The common denominator in each of these cases has been the perceived absence of any signs or symptoms of disease, but distinguishing them is the potential impact of the disease on future health and work.
The importance that future impact of disease plays is clearly highlighted in the platinum salt sensitisation claim of Dryden. Sensitisation was an asymptomatic condition, in this instance, but there was a risk of subsequent allergic reaction (running eyes or nose, skin irritation and bronchial problems) arising with further exposure. It was this future risk (and the impact that it could have on work) which converted the asymptomatic condition into an ‘actionable’ one, yielding compensation:
‘I would distinguish this case from Rothwell … As I see it, it is material that the pleural plaques were nothing more than a marker of exposure to asbestos dust, being symptomless in themselves and not leading to or contributing to any condition which would produce symptoms even if the sufferer were to be exposed to further asbestos dust. Similarly, the sensitization of the claimants in this cases marks that they may have already been exposed to platinum salts, but unlike the plaques, it constitutes a change in their physiological make up which means that further exposure now carries with it the risk of an allergic reaction and for that reason they must change their everyday lives so as to avoid such exposure. Putting it another way, they lost part of their capacity to work or, as the claimants put it in argument, they have suffered a loss of bodily function by virtue of the physiological change caused by the company’s negligence’.
Could asymptomatic COVID-19 infection be distinguished from pleural plaques, as platinum salt sensitisation was?
SECONDARY EXPOSURE COVID-19 CLAIMS?
Secondary exposure claims have long been a feature of asbestos and other occupational disease claims. These claims involve (i) an employer who is at initial fault in exposing an employee to a damaging agent, (ii) the exposed employee exposing family members to the aforementioned agent and (iii) the secondarily exposed family member going on to develop a disease/illness.
In the context of COVID-19 infection claims, if the employer was not at fault in respect of their employee’s exposure to SARS-CoV-2 (primary exposure), then it follows that they would equally not be at fault in respect of any secondary exposure(s).
Conversely, if the employer was at fault in respect of their employee, then considerations relating to the ‘reasonable foreseeability’ of secondary exposure(s) would include:
- How long the employee may have remained infective and/or the virus been live within the family home and onset within the secondary victim?
- Whether the secondary victim could have been exposed elsewhere/likelihood of the same?
- Whether secondary exposure brought about a ‘material increase in risk’ of COVID-19 (depending on the test of causation applied – see section on causation above)?
COVID-19 CLAIMS UNDER THE EMPLOYERS’ LIABILITY (DEFECTIVE EQUIPMENT) ACT 1969?
The Employers’ Liability (Defective Equipment) Act 1969 imposes strict liability on employers for the 3rd party supply of defective equipment, which causes injury to an employee in the course of his/her employment.
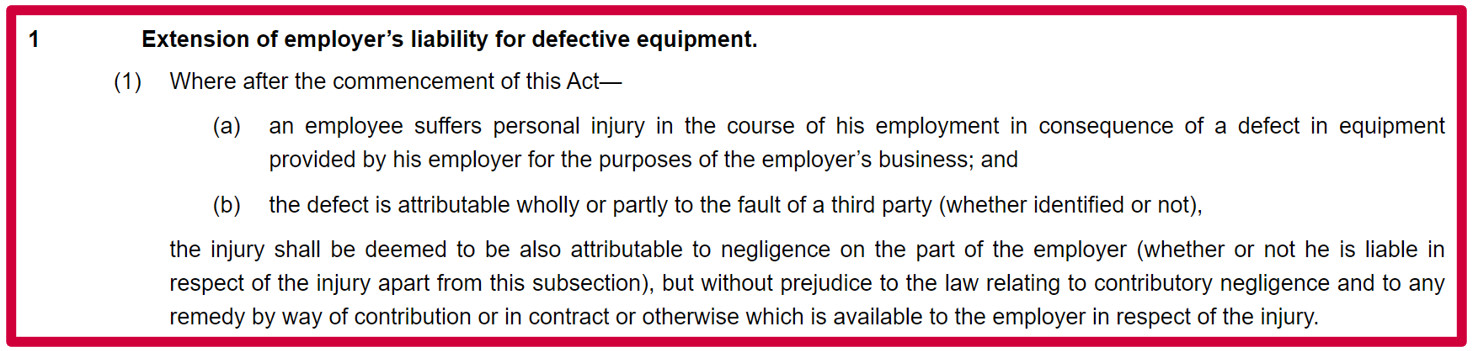
Interestingly, the 1969 Act is versatile enough for its sting to encompass slip/trip claims, i.e. a claim under s.1 would not be limited simply to coronavirus infection claims.
COVID-19 CLAIMS PURSUANT TO THE INDUSTRIAL INJURIES DISABLEMENT BENEFIT SCHEME?
No action has been taken by the Industrial Injuries Advisory Council (IIAC) to classify COVID-19 as a ‘prescribed disease’ eligible for Industrial Injuries Disablement Benefit (IIDB) awards.
For COVID-19 in (a sub-section of) workers to be meet the Council’s threshold of prescription, the ‘relative risk’ of disease would need to be more than 2, i.e. the risk of COVID-19 would need to be doubled for those working in a particular type of job or exposed to SARS-CoV-2 at work.
Only time will tell as to whether COVID-19 is added to Schedule 1 of the Social Security (Industrial Injuries) (Prescribed Diseases) Regulations 1985.
NON-COVID-19 INFECTION INJURIES CAUSED BY THE PANDEMIC?
Musculoskeletal Conditions Among Home Workers?
The shift towards homeworking, amid office closures during the COVID-19 pandemic, has led to a significant increase in new musculoskeletal complaints (neck, shoulder or back pain) and it is accepted that ‘there are going to be questions over whether people can sustain prolonged laptop working’.[130]
Mental Health Conditions Among Home Workers?
Another occupational health risk connected to remote working practices and COVID-19 is stress, alongside other mental health conditions, such as depression and ‘burnout’ (included in the 11th Revision of the International Classification of Diseases as an ‘occupational phenomenon’[131]). The disease is exacerbating work pressures through threat of unemployment, increased workloads, ineffective management and loneliness.[132]
For the leading authority on work-related stress claims, see the then Lady Justice Hale’s list of 16 practical propositions for establishing liability, at para 43 of Sutherland v Hatton [2002] EWCA Civ 76.
Acoustic Shock Among Headset Users?
In recent months, there has been a ‘steep increase’ in Canadian workplace injuries, including acute acoustic shock and tinnitus among remote workers.[133]
This trend has been attributed to workers experiencing problematic sound quality issues with headsets and other communicative devices, e.g. loud feedback loops.[134]
If employers do not provide workers with headsets fitted with acoustic limiters (per the Department of Trade and Industry (DTI) specification 85/013), they may be at risk of noise exposure above 118 dB (130 dB exposure can be acoustic shock-inducing).
Alternatively, workers using limiter-controlled headsets without acoustic shock protection may suffer from ‘central auditory gain’ (increased susceptibility to acoustic shock), which poses more of a risk if feedback is more common than usual, i.e. through workers using cordless phones (which can pick up interference, in the form of static and reduced audio quality[135]), as opposed to their corded office phone.
Legionnaires’ Disease Among Workers Returning from Homeworking?
The HSE and IOSH have warned employers and occupiers that the risk of Legionnaires’ disease may have increased if work premises have been closed or had reduced occupancy throughout the COVID-19 crisis.[136] Infrequent use of water systems during lockdown, could have encouraged legionella growth.
PART 3 – PROCEDURAL AND POLITICAL INFLUENCE
THE PERSONAL INJURY CLAIMS MARKET – A NOTABLE REDUCTION IN INSTRUCTIONS?
On 3 December 2020, the Ministry of Justice (MoJ) published its latest quarterly civil justice statistics for Q3 of 2020 (July to September).[137]

So far this year, a total of 75,338 PI claims have been issued in the county courts, which is representative of an 13% decline compared to the combined total in Q1, Q2 and Q3 of 2019 (86,713).
The COVID-19 pandemic is suspected to have had an impact on these quarterly statistics. Indeed, in Q2 of 2020, just 16,309 personal injury claims were issued in the county courts, which was the 3rd lowest number ever recorded (only Q1 and Q2 of 2009 were lower). The fact that the number of claims issued in Q3 harks back to figures last witnessed in 2017 would seem to imply disjointed claimant behaviour (i.e. due to COVID-19) ahead of mundane seasonal fluctuation.
Of course, the general downward trend of personal injury claims over a number of years can also be attributed in part to civil justice reform enacted through the Legal Aid, Sentencing and Punishment of Offenders Act (LASPO) 2012:
- The abolition of recoverable CFA success fees and ATE insurance premiums;
- A 10% increase in general damages for pain, suffering and loss of amenity;
- A ban on referral fees in respect of personal injury litigation; and
- The introduction of qualified one-way costs shifting (QOCS) in personal injury litigation.[138]
Looking elsewhere at the latest available Compensation Recovery Unit (CRU) registrations data (July to September 2020), obtained by the Association of Consumer Support Organisations (ACSO), it is noticeable that EL/PL claims have been ‘broadly flat on the previous quarter’, but ‘well down compared to the same period last year’ and showing little increase since lockdown.[139]
This has been accredited to the fact ‘many people are still working from home’ and that, should this continue, we could see a fast contraction in personal injury claims across the board.
Finally, casting over to the EL (Disease MI) Claims Portal, the 12-month rolling bar chart of claims notification forms (CNF) sent paints a complementary picture – a general downward trend.[140]
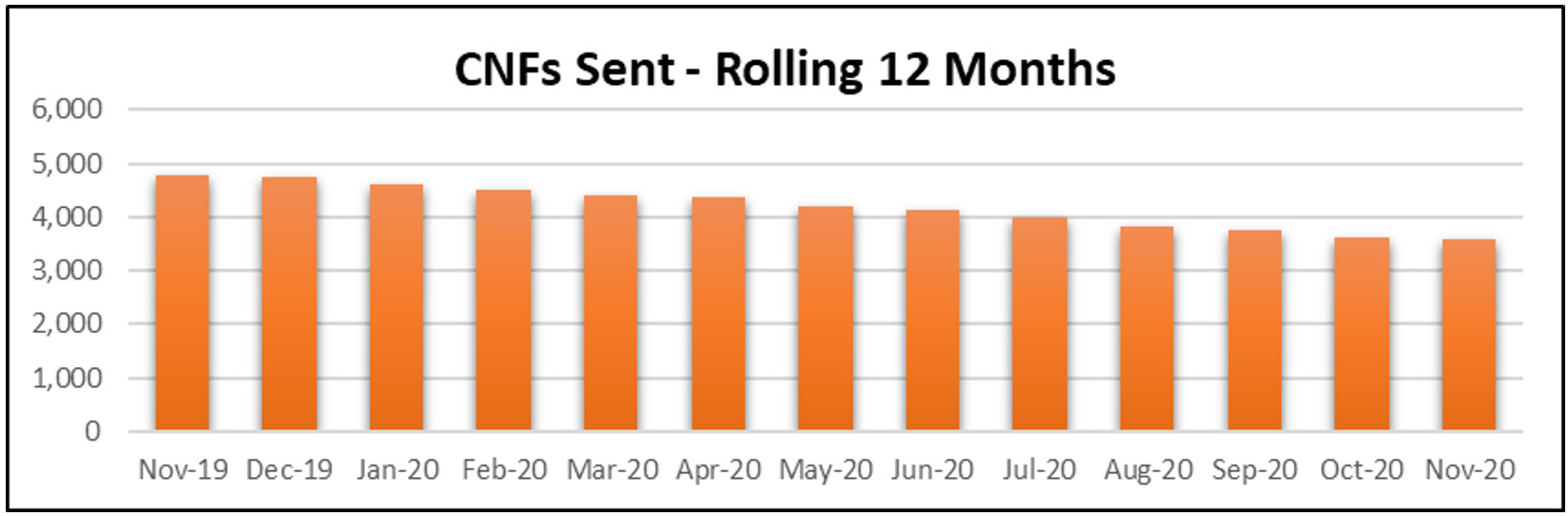
Current estimates suggest that the largest 12 personal injury law firms currently occupy a combined market share of around 30%. Based on this estimate, the personal injury sector is ‘the most heavily concentrated sector’ in the field of consumer law.
Market forecasters, such as IRN Research, have predicted that, at least in the short-term future, to compensate for the drop in claims numbers, the impact of reforms and COVID-19, there will be a rise in individual practice restructuring and diversification; mergers/acquisitions; and more technology-driven solutions introduced at a faster-than-normal rate – see Slater and Gordon’s new ‘automate first’ approach.[141] This has been described as a ‘watershed moment’ for the personal injury sector.[142]
Projections had the total value of the personal injury market falling this year by 1.5% to around £3.92bn. Next year, the value of the personal injury market is not expected to shift upwards or downwards, but 2022 and 2023 are due to foster growth of 2% and 4%, respectively.
Will there be a kick-start to the claims market in 2021? Will it be COVID-19 infection claims that prompt a surge? And will medical examinations, hearings and trials continue to take place on a predominantly remote basis?[143] Only time will tell.
WHIPLASH REFORMS: THE RISE IN SMALL CLAIMS LIMIT
Last year, we informed our readers that the insurance industry had doubts over whether the Ministry of Justice (MoJ) would be able to meet its deadline to bring forward a package of whiplash reforms supplementary to the Civil Liability Act 2018 by April 2020, at the latest.
Such reforms included a rise in the small claims track limit from £1,000 (unamended since 1991) to £5,000 for soft-tissue whiplash claims (and potentially to £2,000 for all other PI claims, including EL/PL claims), alongside a compensation tariff system, a ban on offering/accepting settlement of whiplash claims without first obtaining medical evidence and new IT-based RTA portal infrastructure.
However, in February, the Lord Chancellor and Secretary of State for Justice, the Rt. Hon Robert Buckland QC, announced that the Government would be postponing the implementation of reforms until 1 August 2020, in spite of ‘major progress’ having been made:[144]
‘The government has decided that more time is necessary to make sure the whiplash reform programme is fully ready for implementation. We have always been clear that we need to do this right rather than hastily. In particular, we need to provide sufficient time to work with the Civil Procedure Rules Committee to put in place the supporting rules and pre-action protocol and to give industry sufficient time to prepare their businesses for the changes to how small road traffic personal injury claims are managed. We will also lay the statutory instrument in parliament to introduce the tariff of damages for whiplash injuries’.[145]
Just weeks after this statement was made, the Lord Chancellor was forced, in the early stages of the COVID-19 pandemic, to push back reform even further, admitting that ‘now is not the time to press ahead with significant transformational change to the personal injury sector’.
Consequently, all small claims reforms were deferred until April 2021.[146]
The Government has stressed that it remains ‘firmly committed’ to increasing the small claims track to £5,000 for RTA claims, though the expected increase in litigants in person (due to less claimants being able to recover legal costs) may be a shock to the civil justice system. Nonetheless, consumers are said to be ‘growing in confidence’ to manage their own claims.[147] Meanwhile, only 18% of claimant firms surveyed are ready for the reforms, one being Minster Law, having formally launched its self-service digital claims portal, called INK.[148]
It is becoming increasingly likely, though not at all guaranteed, that all EL/PL claimants will still be legally represented come April 2021, as both claimant and defendant stakeholders have been lobbying against EL/PL reform in recent months – an area which had ‘never’ been identified as a target for reform according to the Association of Business Insurers (ABI).[149]
Even now, though, there is still internal scepticism over the current timetabling. Minutes for the Civil Procedure Rule Committee’s November meeting stated that parties were continuing to ‘work together constructively [on the draft rules], but there is still much to do’.[150]
We do not know when the final version of the new pre-action protocol, practice direction (and draft whiplash injury regulations?) will be published, only that the MoJ is ‘determined’ to do so.[151]
EXTENDING THE FIXED COSTS REGIME
The Ministry of Justice (MoJ) launched a 2-month consultation into extending Sir Rupert Jackson’s fixed recoverable costs scheme in April 2019 and we have been eagerly awaiting the Government’s impending follow-up responses ever since.
Legal commentators had initially predicted some form of update in Autumn 2019 but our forecast in last year’s ‘Horizon Scan’ is still ultimately yet to bear fruit and is now well overdue.
To-date, there has been no official Government publication discussing fixed recoverable costs across all ‘fast track’ claims and ‘intermediate cases’, nor any developments on fixed recoverable costs in a ‘bespoke’ noise-induced hearing loss (NIHL) fast track.
Although it is impossible to say with certainty, in the midst of a global pandemic which has ground all manner of civil justice reform to a halt, the latest intelligence we have implies that the new regime could be in place by October 2021.[152]
In spite of radio silence from the MoJ, it is said that the government department remains ‘very keen’ on following through with its plans, after which it will supposedly begin work on a regime to almost entirely eliminate costs budgeting and post-settlement assessments, i.e. imposing matrices of fixed recoverable costs ‘up to the value of £250,000’.
The changes due to take effect in October 2021 are presented below.
Extended Fast Track and ‘Intermediate Cases’
The upshot of current proposals is that EL/PL disease claims, valued up to £25,000, would be encompassed within the new and expanded fast track. Meanwhile, claims valued between £25,000 and £100,000 would be designated as ‘intermediate cases’ and would be assigned to an ‘extended fast track’.
Mesothelioma and other asbestos-related disease claims would fall outside of a broadened fixed costs regime, as would any claim whose trial is expected to last longer than 3-days, and also where more than 2 expert witnesses are scheduled to give oral evidence.
See the proposed grids of fixed costs, below.
Pre- and Post-Litigated ‘Fast Track Cases’:
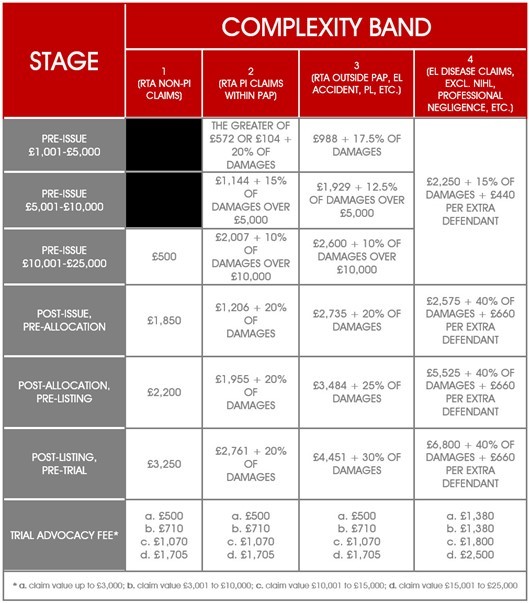
Pre- and Post-Litigated ‘Intermediate Cases’:
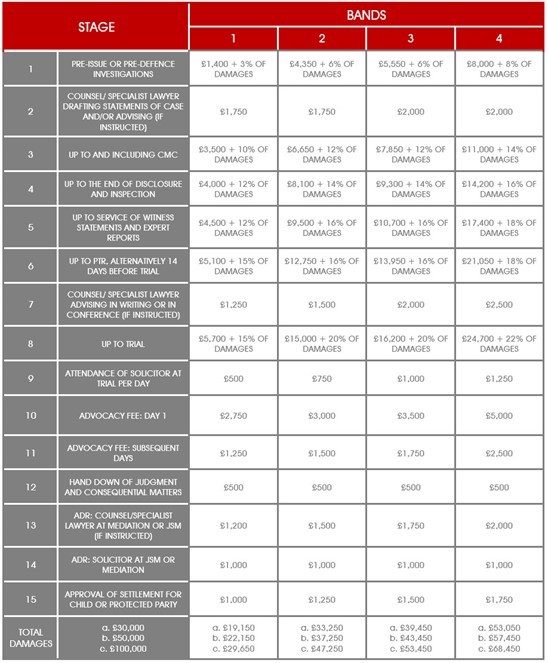
‘Bespoke’ NIHL Fast Track
For NIHL claims, a ‘bespoke’ fast track scheme has been conceived, but the appointed Civil Justice Council (CJC) Working Party pinpointed that certain claims would be exempted (i.e. subject to costs as standard), such as:
- Single defendant cases, where the defendant puts their name on a list for all their cases to commence within the EL/PL portal;
- Single defendant cases commenced within EL/PL portal, which subsequently fall out of the portal;
- Military claims;
- Claims valued at more than £25,000;
- Claims with more than 3 defendants; and
- Claims where a defendant, in their letter of response:
- Argues that the work-related hearing loss is de minimis;
- Submits a request for a repeat audiometry;
- Submits a request for own medical evidence (ENT Consultant, etc.); or
- That the claim is to be treated as a ‘test case’ (the scope of this has not been agreed).
For eligible claims, expected costs [exclusive of VAT, reasonable disbursements (but not counsel fees) and restoration fees (£1,280 per defendant excl. VAT)] are displayed in the tables below:
Pre-Litigated NIHL Claims:
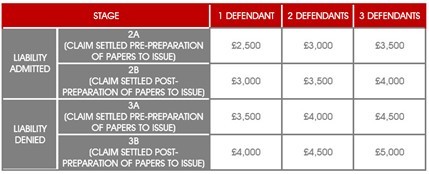
Litigated NIHL Claims:
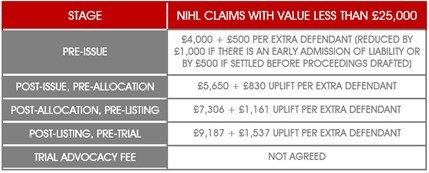
In 2017, we compared current defence spend against fixed fee spend, the results of which were best illustrated by the table below:

USING THE NEGATIVE DISCOUNT RATE
For over a year, in England and Wales, the personal injury discount rate (otherwise known as the ‘Ogden rate’), which is used to calculate lump sum damages for future losses in high value personal injury claims, has been set at (-)0.25%. Meanwhile, Scotland’s discount rate has been fixed at (-)0.75%.
Contrary to our predictions in last year’s ‘Horizon Scan’, there has been no indication that claimants are employing ‘forum shopping’ tactics; that is to say where claimants, who are eligible to bring personal injury claims in multiple UK jurisdictions, choose to advance proceedings where the discount rate is lowest, i.e. where it is assumed that the claimant will receive a lower return from its invested damages.
Several months ago, we became aware that that the insurance market would not be pursuing a judicial review challenge of the new discount rate in England and Wales, quelling concerns that we voiced in 2019. That being said, in recent weeks, the Association of Personal Injury Lawyers (APIL) has announced that it will be launching a judicial review challenge of Northern Ireland’s decision not to set an interim discount rate, pending its pledge to introduce a new mechanism for setting the rate (potentially in line with Scotland) through legislation. According to APIL’s spokesperson for Northern Ireland, ‘a formal letter to the Northern Ireland Department of Justice with a view to making an application for a judicial review of the decision announced in October should it remain unchanged’.[153]
One of the ways in which the negative personal injury discount rate made waves this year was in the case of Swift v Carpenter & Anor [2020] EWCA Civ 1295, which we analysed in edition 318 (here).
When claimants sustain life-changing physical injuries that impair mobility, their pre-injury accommodation is often no longer suited to their post-injury requirements and new accommodation is sought. It is normal for new accommodation to exceed the value of the victims’ previous accommodation.
Following the longstanding Roberts v Johnstone approach, courts have historically not awarded claimants the value of the new accommodation.
Instead, they compensated claimants for the annual loss of income brought about by spending their own money on accommodation, in preference to making investments, using the following 2-stage calculation:
Step 1: Multiply the capital property cost (the difference between the value of the old and new accommodation) by the prevailing personal injury discount rate.
Step 2: Multiply the figure from Step 1 by the multiplier for pecuniary loss of life (using Tables 1 and 2 of the Ogden Tables).
E.g., under the previous 2.5% discount rate (effective up to 2017), a 51-year-old male claimant moving from a £300,000 home to a £550,000 home would have received:

Ordinarily, during times when a positive personal injury discount rate was in force, this was fair, because awarding claimants the full capital cost of special accommodation would eventually result in over-compensation by the time that the claimant died, i.e. the value of the asset would be expected to have enhanced.
Any deficit (in the example above: £250,000 - £139,187.50 = £110 812.50) was typically topped up by damages for other heads of loss (invariably general damages).
However, since 2017, when the personal injury discount rate was negativised, McGregor on Damages (19th Edition) was correct to prophesise that ‘the Roberts v Johnstone method becomes unworkable; it would produce a nil award’.
The reason for this is plainly that the multiplicand in the Roberts v Johnstone formula can only be generated if the assumed rate of return is at or above 0%.
Devising a ‘fair and proper solution’ to the reality that some victims of serious personal injury would, in the absence of substantial general and special damages and ‘nil’ Roberts v Johnstone awards, be left with ‘no prospect at all of obtaining special accommodation which they ought to have’, Lord and Lady Justices Irwin, Davies and Underhill unanimously overturned the Roberts v Johnstone methodology.
In its place, it was considered appropriate, in a negative discount rate era, to compensate the claimant for the capital value of new accommodation, less ‘reversionary interest’, i.e. the value of the ‘windfall’ that would be accrued by a claimant over a prolonged time period, given a projected rate of return on the investment (‘discount rate’).
In Swift, the claimant in this action suffered leg injuries in a road-traffic accident (RTA), which resulted in a below-knee amputation and the need for larger accommodation, at a cost of £900,000. She was 43-years-old at the date of trial [43.58-years-old for the purpose of Ogden (7th edition)]. The discount rate was set at 5%:

To our knowledge, the defendants in Swift are seeking the Court of Appeal’s permission to take the case to the Supreme Court and this is something to look out for in future editions of BC Disease News.
Until an appeal is heard, though, it is safe to say that awards in majority of ongoing cases in 2021 will increase under the ‘reversionary interest’ approach, with practitioners and insurers likely reviewing their schedules of loss and offers of settlement upwards.
EXTENDING ELIGIBILITY FOR BEREAVEMENT DAMAGES
In last year’s ‘Horizon Scan’, we predicted that there would be some progression with the Government’s proposed Fatal Accidents Act 1976 (Remedial) Order, which asserted that ‘a claimant who cohabited with the deceased person for a period of at least two years immediately prior to the death’ would be able to pursue a claim for ‘bereavement’ damages.
Laid before Parliament on 12 February 2020, the draft Order, was supposed to remedy the Court of Appeal’s judgment in Smith v Lancashire Teaching Hospitals NHS Foundation Trust & Ors (Rev 2) [2017] EWCA Civ 1916, as s.1A(2) of the Act had been declared incompatible with the European Convention of Human Rights (ECHR), pursuant to s.4 of the Human Rights Act 1998:
‘... in the context of bereavement damages under section 1A of the FAA, the situation of someone like Ms Smith, who was in a stable and long term relationship in every respect equal to a marriage in terms of love, loyalty and commitment, is sufficiently analogous to that of a surviving spouse or civil partner to require discrimination to be justified in order to avoid infringement of Article 14 in conjunction with Article 8 [of the European Convention on Human Rights] … it is the intimacy of a stable and long term personal relationship, whose fracture due to death caused by another’s tortious conduct will give rise to grief which ought to be recognised by an award of bereavement damages, and which is equally and analogously present in relationships involving married couples and civil partners and unmarried and unpartnered cohabitees’.
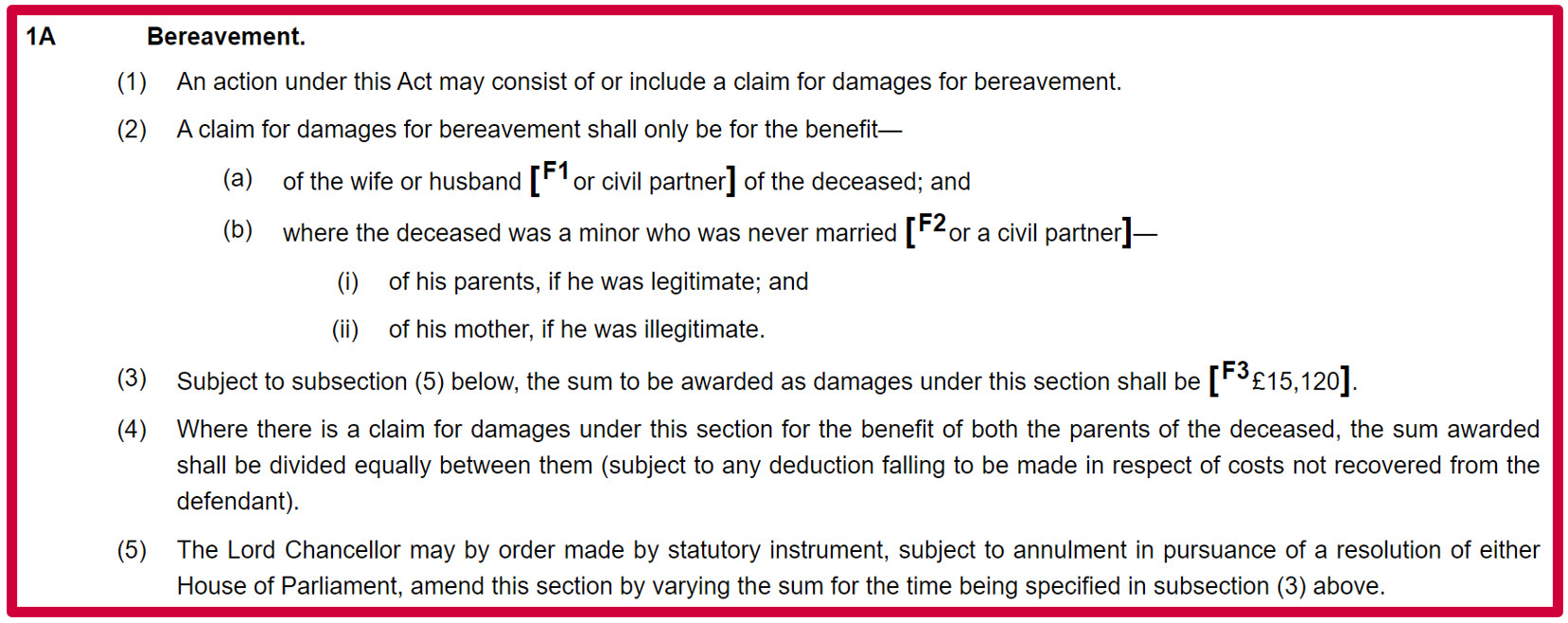
The draft Order was approved by the House of Commons on 15 June 2020, shortly after the Joint Committee on Human Rights, which had been tasked with scrutinising the Order under the ‘non-urgent’ procedure, published its 2nd Report (dated 18 May 2020) and reiterated its recommendation for a consultation on wider reform of s.1A ‘to ensure it is fully compliant with human rights law and reflects the reality of modern family life’ – read our full article in edition 308 (here).
At that time, the Joint Committee was ‘disappointed’ that the Government had rejected any further consultation on the bereavement damages scheme because it considered that the list of eligible claimants in its present form is ‘still vulnerable to human rights challenges’, e.g.:
‘… fathers grieving the loss of children born outside of wedlock; parents grieving the loss of adult or married children; children grieving the loss of a parent; and siblings grieving the loss of a brother or sister’.
The Joint Committee was also quizzical over whether the equivalent Scottish model of assessing damages for ‘loss of society’ (under the Damages (Scotland) Act 2011), on a case-by-case basis, would present a fairer alternative for England & Wales than its fixed lump sum model.
Many of these concerns were regurgitated at the Grand Committee of the House of Lords, on 3 September 2020:[154]
‘… the noble Lord, Lord Hain, spoke about the provision for couples that may be together but not sharing a home …
A number of noble Lords, including the noble and learned Lord, Lord Falconer, mentioned that no provision is made for couples who have lived together for less than two years. The period of two years already applies in other cases; certainly, under Section 1(3)(b) of the 1976 Act, the Court of Appeal did not question the validity of the two-year period …
Several noble Lords brought up the fact that the law is not the same in England as in Scotland …
The noble Lord, Lord Hain, also asked why this measure is not in primary legislation …
… the Scottish system and primary legislation … was brought up by the noble Lord, Lord Thomas of Gresford.
The noble and learned Lord, Lord Falconer … talked about … the issue about a father and the loss of a child …
There has been a lot of talk from noble Lords about the Act itself, including how old it is and the fact that some of it uses inappropriate language, as we heard from the noble Baroness, Lady Jones of Moulsecoomb’.
In spite of these remarks, Baroness Scott of Bybrook maintained that the draft Order ‘accurately and effectively’ rectified the incompatibilities identified by the Court of Appeal in Smith and confirmed that it would be brought into effect ‘as swiftly as possible’.
And indeed it was, with The Fatal Accidents Act 1976 (Remedial) Order 2020 having been made on 15 September and entering into force on 6 October 2020. It is important to note that the Order does not apply retrospectively, i.e. it only applies to causes of action which accrue on or after the date of enforcement.
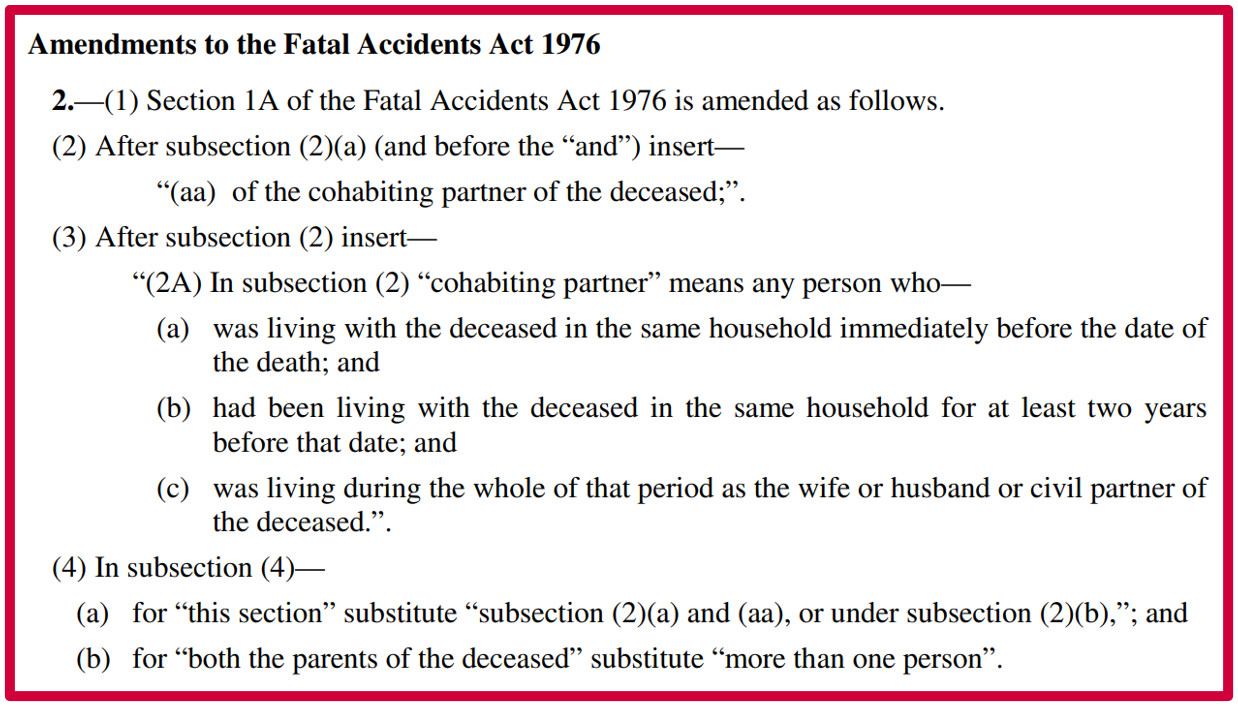
Concurrently this year, ‘damages for bereavement’, has also increased to £15,120 (from £12,980) for cases with causes of action accruing on or after 1 May 2020. This was effected by The Damages for Bereavement (Variation of Sum) (England and Wales) Order 2020 (laid before Parliament on 19 March 2020) – we reported this in edition 306 (here).
The law in England and Wales is now in line with the position in Northern Ireland (£15,100 since May 2019).
Nonetheless, in the year ahead, it will be interesting to see whether the Government seeks wholesale reform, per the Joint Committee’s requests and demands from the Association of Personal Injury Lawyers (APIL). If so, this will therefore require primary legislation.
6-YEAR LONGSTOP FOR MILITARY DISEASE CLAIMS: OPERATIONS (SERVICE PERSONNEL AND VETERANS) BILL
As we first reported, in edition 311 of BC Disease News (here), Part 2 of the Overseas Operations (Service Personnel and Veterans) Bill will (pending Royal Assent) amend s.33 of the Limitation Act 1980 to limit the court’s discretionary power to disapply time limits for civil claims brought against the Ministry of Defence (MoD) by (ex-)service personnel, in respect of personal injuries or death, which relate to overseas operations of the armed forces (‘overseas armed forces actions’).
More specifically, this piece of draft legislation would insert, into s.33(1) of the 1980 Act, the clause:
‘The court shall not under this section disapply any provision of section 11 in its application to an overseas armed forces action if the action was brought after the expiration of the period of six years from the section 11 relevant date’ (pursuant to Schedule 2 of Part 1 of the Bill).
In practice, what would this 6-year longstop mean for a soldier who wished to commence legal action after developing a condition with a long latency period, such as post-traumatic stress disorder (PTSD), noise-induced hearing loss or mesothelioma, owing to exposure in the course of their employment outside of the British Islands?
Well, as usual, they would have 3-years from their ‘date of knowledge’ (this would ordinarily be acquired later than the ‘cause of action’ in such claims) to bring a claim in time.
Thereafter, they would have 3-years to bring a claim out of time (i.e. after the limitation period is deemed to have expired), subject to the success of a s.33 application.
Once 6-years from the ‘date of knowledge’ has elapsed, the Courts would no longer have jurisdiction to hear the claim on an indefinite basis. That being said, the claimant would (if they had not already) hypothetically still benefit from an additional 365-days to seek redress under the no-fault Armed Forces Compensation Scheme (AFCS), which sets a 7-year limitation period.
The purpose of this new Bill is supposedly to ‘stop vexatious and repeated claims’ against the MoD, as opposed to circumventing or frustrating the ability to bring military compensation claims.
However, the Bill has not escaped criticism, with the Law Society recently having warned that the proposed constriction of s.33 discretion may lead to ‘gross injustice’:
‘Only the MoD stands to gain from the proposed time limit on compensation claims, as it would avoid having to pay court-awarded damages and costs. If claims are blocked by the bill the MoD would also be less likely to learn from past mistakes and improve practices’.
Whilst the Government Bill was started in the Commons, it has now reached its 2nd reading in the House of Lords. The date of this reading is yet to be announced, but will likely take place sometime in the new Year.
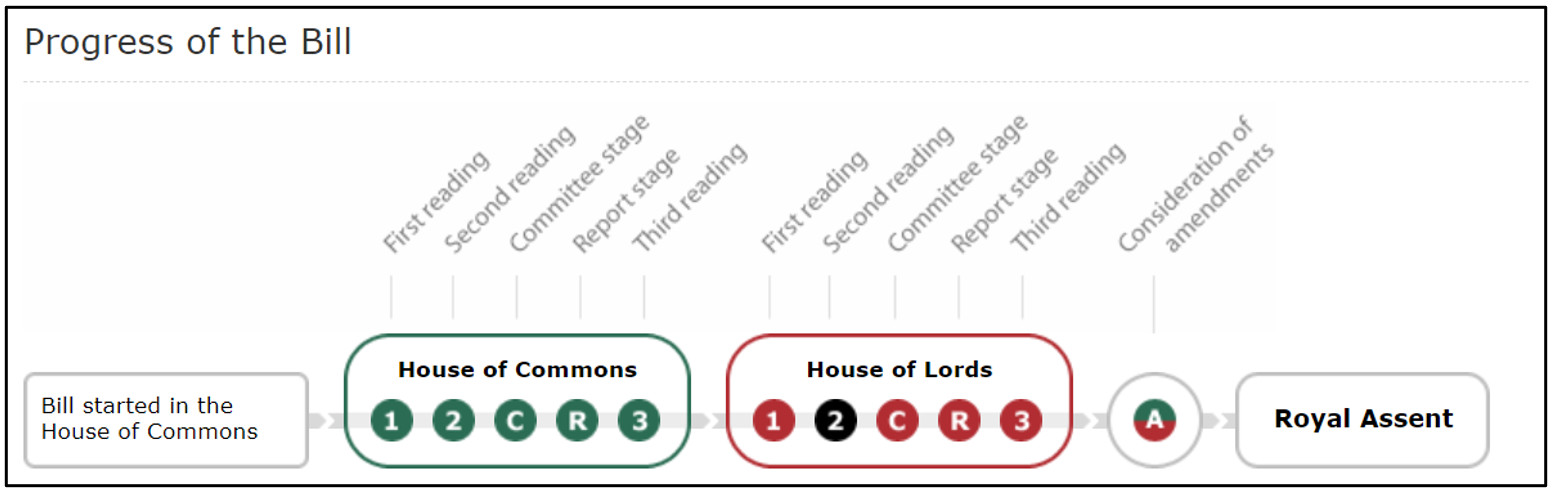
LIABILITY FOR NHS CHARGES (TREATMENT OF INDUSTRIAL DISEASE) (SCOTLAND) BILL
Ancillary to the Overseas Operations (Service Personnel and Veterans) Bill, which was a new legislative proposal for 2020, another new draft law to enter the fore this year was the Liability for NHS Charges (Treatment of Industrial Disease) Scotland Bill.
Even though we had, on several previous occasions over the past couple of years, theorised that such a proposal could be made, it was not until recently that the Bill was formally introduced through the Scottish devolved Parliament.
If the Bill were to receive Royal Assent, it would ‘enable Scottish Ministers to recover, from the party responsible for causing an industrial disease, certain costs incurred by the NHS in providing care and treatment to those suffering from that disease’ – in other words, increased liability for paying defendants.
Simply put, the Bill would overturn s.150(5) of the Health and Social Care (Community Health and Standards) Act 2003 – a provision which prevents there from being a mechanism through which NHS charges can be recouped from negligent employers (or their insurers) for the treatment of ‘primary diseases’ (excluding diseases that spur from an ‘accident’) sustained by claimant employees, which result from tortious exposures in the workplace.
In edition 311 (here), we reported that by 30 September 2020, the Health and Sport Committee would close its ‘call for views’ on the Bill in its extant form, namely:
- How the Bill will lead to improved working conditions and health and safety practices in workplaces;
- How the Bill will help prevent industrial diseases in the future; and
- What impacts the Bill will have on (i) individuals, (ii) NHS boards, (iii) workplaces and (iv) the insurance industry.[155]
It is foreseeable that the Bill will progress through various stages of parliamentary scrutiny in 2021 and we will pay increased attention to Westminster debates in Hansard, on the proviso that ministers may be incentivised to establish a level playing field across the UK. Alternatively, Scottish ministers may be obliged to turn down the NHS Charges Bill in view of the judgment in Aviva Insurance Ltd & Anor, R (On the Application Of) v The Secretary of State for Work and Pensions [2020] EWHC 3118 (Admin) – the corresponding case comment is the 2nd article of this edition.
REVIEW OF SOLICITORS’ GUIDELINE HOURLY RATES
Fast approaching at the turn of 2020, ‘optimistically’ speaking, we should be able to report that recommendations from a review of Solicitors’ Guideline Hourly Rates (GHR), conducted by the Civil Justice Council’s (CJC) GHR Working Group, has been published.
Historically, GHR were always ‘locally-derived’, i.e. based on information collated by practising district judges and solicitors, in their respective county courts.
However, in conjunction with the Civil Procedure Rules coming into force in 1999, the Supreme Courts Costs Office (SCCO) published a Guide in 2002, laying out GHR on a national scale.[156]
In 2014, 2010-established GHR were frozen indefinitely and are thus effective today, separated by experience (‘Bands’ A-D) and location (‘London’ and ‘National’ Grades).
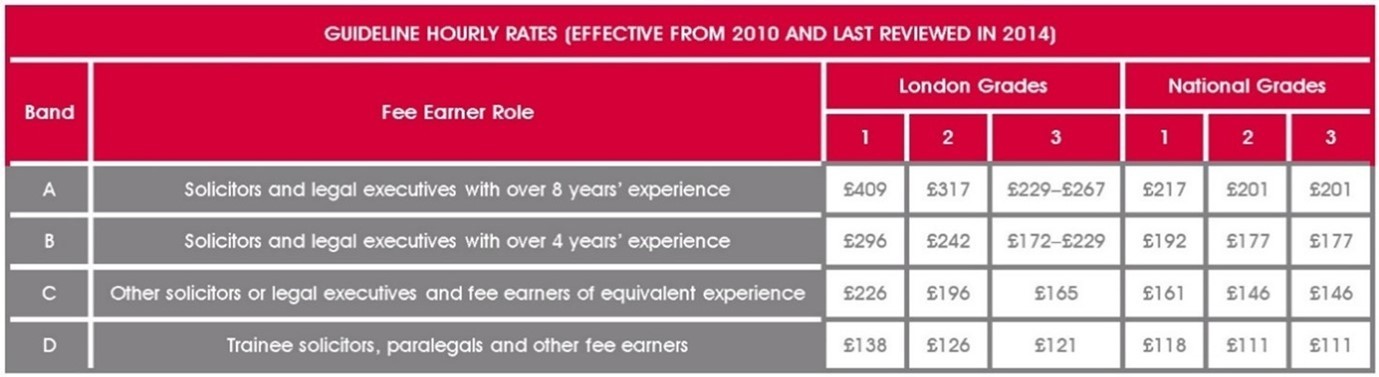
However, in December 2019, the CPRC costs sub-committee published a report, criticising the 2014 review for seeking to rigorously establish ‘actual rates to a high degree of accuracy’, sooner than form ‘broad approximations of actual rates in the market’.
Pressure to bring about reform was also ‘welcomed’ by Mrs. Justice O’Farrell, in the case of Ohpen Operations UK Ltd v Invesco Fund Managers Ltd [2019] EWHC 2504 (TCC), who branded present guidelines ‘unsatisfactory’.
While the GHR review has been ongoing this year, swathes of litigators had been inspired by the landmark ruling in PLK & Ors (Court of Protection:Costs) [2020] EWHC B28 (Costs), wherein Costs Master Whalan (who was not personally empowered to review or amend GHR) inflated costs by 20% above current GHR, to request similar outcomes ‘across the board’ (i.e. not restricted to Court of Protection actions) – an ‘unprecedented step’ became spill-over litigation, as we reported in edition 316 (here).
We have since reported (here), similarly, on the case of Cohen v Fine & Ors [2020] EWHC 3278 (Ch), in which His Honour Judge Hodge QC found that GHR ‘should be the subject of, at least, an increase that takes due account of inflation’, increasing figures ‘in the order of 35% … as a starting point (appropriately rounded-up for ease of calculation)’.
CONTEMPT OF COURT AND CLAIMS FRAUD
Where 2019 was a year steeped in anti-fraud measures, civil contempt proceedings and findings of ‘fundamental dishonesty’, pursuant to CPR 44.16 and s.57 of the Criminal Justice and Courts Act 2015, 2020 has been comparatively meagre.
As with many of the themes discussed in this feature article, we can attribute the lack of content to the COVID-19 claims environment.
Nonetheless, in edition 314 (here), we discussed an important section of the 122nd Update to the Practice Directions, through which the Civil Procedure Rule Committee (CPRC) amended PD 35 para 3.3 on experts’ signed statements of truth, from 1 October 2020 onwards.
Ultimately, the Practice Direction has been modified to the effect that it now compels experts to produce more extensive signed statements, which recognise the risk of contempt applications being lodged against them, should applicants accuse them of having been dishonest.
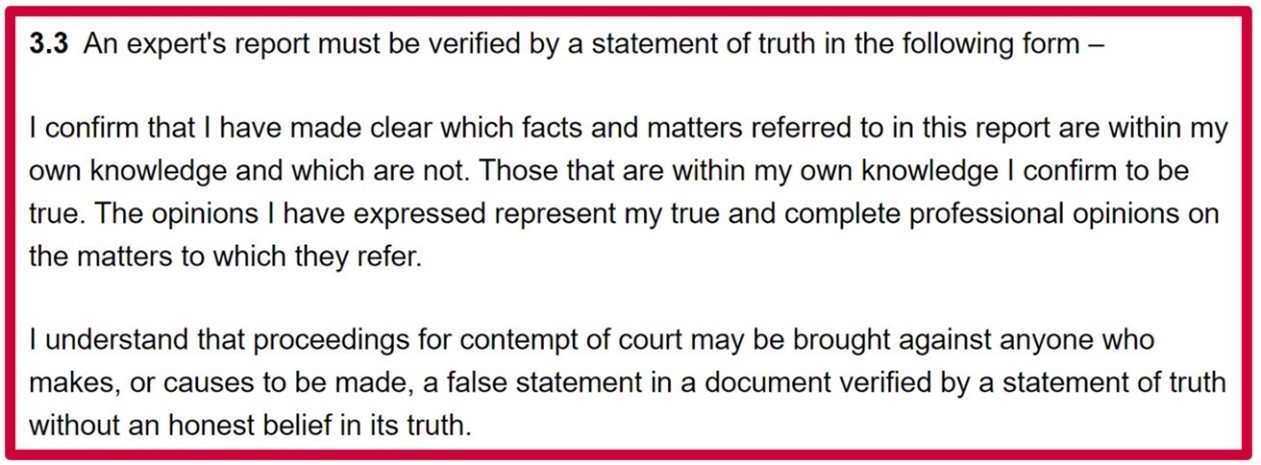
The impetus for this amendment was, by and large, the case of Liverpool Victoria Insurance Company v Khan [2019] EWCA 392 (Civ), which featured in last year’s ‘Horizon Scan’, in which a motor insurer successfully brought a committal action against Dr. Asef Zafar, a medical expert who ‘recklessly’ drafted a fraudulent medical report for a road-traffic accident (RTA) claimant by exaggerating the claimant’s symptoms.
In that specific instance, the Court of Appeal found ‘little difference in culpability’ between ‘reckless’ fraud and ‘intentional’ fraud and therefore ruled that the lower court should have stipulated a custodial sentence ‘significantly longer than 6 months’, which should not have been suspended.
The new PD 35 para 3.3 should hypothetically contribute towards a dampening influence of claims fraud in 2021, as the personal injury market is exposed to reforms that might otherwise entice claimants to pursue fraudulent tactics for financial gain.
STANDARDS OF EXPERTS
On the topic of medical experts, in last year’s ‘Horizon Scan’, we stated that we would continue to monitor discussions between the Association of Personal Injury Lawyers (APIL) and the Forum of Insurance Lawyers (FOIL), throughout 2020, as they deliberate over a protocol governing the recording of medico-legal examinations.
Of course, this was in relation to comments made by Master Davison, in the case of Mustard v Flower & Ors [2019] EWHC 2623 (QB), imploring both parties to ‘give attention to’ an agreed protocol as a means to address the issue of parties admitting ‘covertly’ (but not necessarily ‘unlawfully’) recorded evidence:
‘It is the interests of all sides that examinations are recorded because from time to time significant disputes arise as to what occurred. In that situation, it is important to have a complete and objective record of the examination, which is subject to appropriate safeguards and limitations on its use. It is desirable that the parameters of such recording should be on an "industry-wide" agreed model which caters for the many issues capable of arising and, I might add, which pays careful attention to the containment of the costs that might potentially be generated.
... an APIL / FOIL agreed protocol is the way forward. Such a protocol would provide an agreed scheme for the recording of examinations and for the reception of such evidence. There would then be no need or incentive for covert recording so that such cases would be unlikely to arise in the future. If they did arise, the protocol would dictate or steer the outcome of an application such as the present one. I hope that the relevant organisations can give attention to this topic in the future’.
Sure enough, we reported earlier this year (here) that a joint working party had been created so that APIL and FOIL could devise an answer to this issue, while the British Psychological Society (BPS) began the process of developing its own guidelines (for neuropsychologists and other professionals).
We also reported that Mr. Justice Spencer had echoed support for an APIL/FOIL-agreed protocol, in the case of Macdonald v Burton [2020] EWHC 906 (QB) and that there should be a ‘level playing field’ between claimant and defendant experts of all disciplines:
‘I hope that the BPS and the joint working party of APIL and FOIL will together work through these issues and come up with a solution which satisfies the interests of justice from the point of view of both claimants and defendants, and I would hope that that would allow for recording of some kind in certain cases. But in my judgment it is not appropriate for me to lay down any kind of ex cathedra guidelines or instructions in relation to that at this delicate stage’.
Spencer J reflected that it would be ‘disappointing’ if forthcoming guidelines were to ban all recordings, as they can offer the clear forensic advantage of disinterring ‘lack of competence of certain experts’ – expert competency being a frequently debated topic among practitioners and judges (this year being no exception).
[1] Helen Coffey, ‘JETBLUE PILOT WINS LANDMARK COMPENSATION CASE AGAINST AIRLINE AFTER GETTING ILL FROM CONTAMINATED AIR’ (12 August 2020 The Independent) <https://www.independent.co.uk/travel/news-and-advice/jetblue-pilot-captain-compensation-contaminated-air-toxic-airbus-plane-oil-fumes-a9667076.html> accessed 21 December 2020.
[2] Mike Wright, ‘US plane toxic fume case victory 'a great step forward' for UK cabin crews as high court battle looms’ (31 August 2020 The Telegraph) <https://www.telegraph.co.uk/news/2020/08/31/us-plane-toxic-fume-case-victory-great-step-forward-uk-cabin/> accessed 21 December 2020.
[3] Hajera Blagg, ‘Landmark toxic cabin air ruling’ (14 August 2020 Unite Live) <https://unitelive.org/landmark-toxic-cabin-air-ruling/> accessed 21 December 2020.
[4] ‘Bayer agrees to $10.9bn settlement over Monsanto’s weedkiller Roundup’ (24 June 2020 The Guardian) <https://www.theguardian.com/business/2020/jun/24/bayer-109bn-settlement-monsanto-weedkiller-roundup> accessed 21 December 2020.
[5] Sean Poulter, ‘B&Q will stop selling weedkiller Roundup after cancer link discovered in the US’ (22 May 2020 Daily Mail) <https://www.dailymail.co.uk/news/article-8349041/B-Q-stop-selling-weedkiller-Roundup-cancer-link-discovered-US.html> accessed 21 December 2020.
[6] Jef Feeley, ‘J&J to Pay More Than $100 Million to End Over 1,000 Talc Suits’ (5 October 2020 Bloomberg) <https://www.bloomberg.com/news/articles/2020-10-05/j-j-to-pay-more-than-100-million-to-end-over-1-000-talc-suits> accessed 21 December 2020.
[7] Jonathan Stempel, ‘Johnson & Johnson fails to overturn $2.12 billion baby powder verdict, plans Supreme Court appeal’ (3 November 2020 Reuters) <https://uk.reuters.com/article/uk-johnson-johnson-talc-ruling/johnson-johnson-fails-to-overturn-2-12-billion-baby-powder-verdict-plans-supreme-court-appeal-idINKBN27J2N6> accessed 23 December 2020.
[8] ‘Johnson & Johnson to stop selling baby powder in US and Canada’ (19 May 2020 The Guardian) <https://www.theguardian.com/business/2020/may/19/johnson-johnson-baby-powder-us-canada> accessed 21 December 2020.
[9] ‘J&J to sell baby powder in UK despite stopping US sales’ (20 May 2020 BBC) <https://www.bbc.co.uk/news/business-52732755> accessed 21 December 2020.
[10] Eric Sagonowsky, ‘Johnson & Johnson's $2B talc verdict stands after Missouri Supreme Court turns away its appeal’ (4 Noveber 2020 Fierce Pharma) <https://www.fiercepharma.com/pharma/j-j-faces-2-11b-talc-verdict-after-missouri-supreme-court-denies-reviewing-its-appeal> accessed 22 December 2020.
[11] ‘British woman can bring asbestos cancer claim in New York against Clinique and Estee Lauder’ (4 May 20202 Leigh Day) <https://www.leighday.co.uk/News/Press-releases-2020/May-2020/British-woman-can-bring-asbestos-cancer-claim-in-N> accessed 21 December 2020.
[12] David Platt QC, ‘David Platt QC obtains landmark judgment in low-exposure asbestos claim: Bannister v Freemans Plc’ (19 May 2020 Crown Office Chambers) <https://www.crownofficechambers.com/2020/05/19/david-platt-qc-obtains-landmark-judgment-in-low-exposure-asbestos-claim-bannister-v-freemans-plc/> accessed 21 May 2020.
[13] Fairchild v Glenhaven Funeral Services Ltd & others [2002] UKHL 22.
[14] ‘Cutaneous malignant melanoma and occupational exposure to (natural) UV radiation in pilots and aircrew’ (May 2020 GOV.UK) <https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/883556/cutaneous-malignant-melanoma-and-occupational-exposure-to-uv-radiation-in-pilots-and-aircrew-iiac-report.pdf> accessed 21 December 2020.
[15] Maria Dinzeo, ‘Apple Dodges IPhone Radiation Class Action Suit’ (29 October 2020 Courthouse News Service) <https://www.courthousenews.com/apple-dodges-iphone-radiation-class-action-suit/> accessed 22 December 2020.
[16] ‘Faster footballs result in harder headers’ (13 October 2020 University of Leeds) <https://www.leeds.ac.uk/news/article/4673/faster_footballs_result_in_harder_headers> accessed 30 October 2020.
Tierney GJ et al., Force experienced by the head during heading is influenced more by speed than the mechanical properties of the football. Scandinavian Journal of Medicine & Science In Sports (2020) <https://onlinelibrary.wiley.com/doi/epdf/10.1111/sms.13816> accessed 30 October 2020.
[17] Charlie Walker, ‘Modern footballers heading 80mph balls “are JUST as much at risk of dementia as the generation of Jeff Astle, Nobby Stiles, and Bobby and Jack Charlton who played with the old, leather balls”’ (3 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8906019/Footballers-just-risk-dementia-Jeff-Astle-Bobby-Charlton.html> accessed 20 December 2020.
[18] Caroline Wilson, ‘Football headers led to “working memory” decline’ (18 November 2020 Herald Scotland) <https://www.heraldscotland.com/news/18879778.football-headers-led-working-memory-decline/> accessed 20 December 2020.
Jonathan Chadwick, ‘Heading a football just 20 times could lead to reduced brain function and signs of concussion, study finds’ (18 November 2020 Daily Mail) <https://www.dailymail.co.uk/sciencetech/article-8962121/Heading-football-just-20-times-lead-reduced-brain-function.html> accessed 20 December 2020.
Ashton J et al., Immediate effects of an acute bout of repeated soccer heading on cognitive performance. Science and Medicine in Football. (31 October 2020) <https://www.tandfonline.com/doi/full/10.1080/24733938.2020.1846769?journalCode=rsmf20> accessed 20 December 2020.
[19] Jeremy Wilson, ‘Research shows increased heading at international level since 1960s, adding to pressure to act over dementia risk’ (26 November 2020 The Telegraph) <https://www.telegraph.co.uk/football/2020/11/26/research-shows-increase-heading-international-level-since-1960s/> accessed 3 December 2020.
Warren Manger, ‘Today’s footballers “at greater risk of brain disease as they head ball more now”’ (26 November 2020 The Mirror) <https://www.mirror.co.uk/sport/football/news/todays-footballers-at-greater-risk-23076325> accessed 3 December 2020.
[20] Sam Peters, ‘There may be changes off the field in dementia research after Jeff Astle's tragic death from heading a ball repeatedly, but changes on it are likely to be painfully slow’ (21 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8973905/There-changes-field-Jeff-Astles-death-changes-slow.html> accessed 22 December 2020.
[21] Martyn Ziegler, ‘Don’t ban heading – nothing has been proved’ (21 December 2020 The Times) <https://www.thetimes.co.uk/article/dont-ban-heading-nothing-has-been-proved-q6bnqz5d7> accessed 21 December 2020.
[22] ‘Football and dementia: Alan Jarvis' death “caused by heading balls”’ (15 October 2020 BBC) <https://www.bbc.co.uk/news/uk-wales-54561861> accessed 27 October 2020.
David Banner, ‘Heading footballs contributed to Welsh player's dementia, inquest concludes’ (16 October 2020 Shropshire Star) <https://www.shropshirestar.com/news/local-hubs/mid-wales/2020/10/16/heading-balls-contributed-to-former-footballers-dementia-inquest-concludes/> accessed 27 October 2020.
Jeremy Wilson, ‘Alan Jarvis died from dementia caused by heading footballs, inquest finds’ (15 October 2020 The Telegraph) <https://www.telegraph.co.uk/football/2020/10/15/alan-jarvis-died-dementia-caused-heading-footballs-inquest-finds/> accessed 27 October 2020.
[23] ‘Football and dementia: Alan Jarvis' death “caused by heading balls”’ (15 October 2020 BBC) <https://www.bbc.co.uk/news/uk-wales-54561861> accessed 20 December 2020.
[24] ‘Dementia in football – should it be recognised as an industrial disease?’ (17 November 2020 Sky News) <https://news.sky.com/story/dementia-in-football-should-it-be-recognised-as-an-industrial-disease-12133458> accessed 20 November 2020.
[25] Mike Keegan, ‘REVEALED: Nobby Stiles' dementia WAS caused by heading - with England and Manchester United legend's family “angered and vindicated” after being informed by leading doctor who examined World Cup winner's brain’ (20 December 2020 Daily Mail) https://www.dailymail.co.uk/sport/sportsnews/article-9073385/Nobby-Stiles-dementia-caused-heading-says-leading-doctor.html> accessed 20 December 2020.
[26] ‘Premier League managers want heading curbed if it leads to dementia’ (20 November 2020 Reuters) <https://in.reuters.com/article/soccer-england-dementia/update-1-soccer-premier-league-managers-want-heading-curbed-if-it-leads-to-dementia-idINL1N2I622I> accessed 20 December 2020.
James Robson, ‘Dementia in football: Chelsea may restrict heading in training as Frank Lampard calls for more research’ (19 December 2020 Evening Standard) <https://www.standard.co.uk/sport/football/chelsea/dementia-in-football-chelsea-may-restrict-heading-in-training-frank-lampard-b74385.html> accessed 20 December 2020.
Dementia in football: Sir Geoff Hurst supports ban on children heading balls’ (18 November 2020 The Guardian) <https://www.theguardian.com/football/2020/nov/18/dementia-in-football-sir-geoff-hurst-supports-ban-on-children-heading-balls> accessed 20 December 2020.
‘Football and dementia: Steve Bruce says there is a “genuine concern” about possible link’ (20 November 2020 BBC) <https://www.bbc.co.uk/sport/football/55007926> accessed 20 December 2020.
Aston Villa manager Dean Smith admits concern over links with heading and dementia (19 December 2020 Sky Sports) <https://www.skysports.com/football/news/11677/12136106/aston-villa-manager-dean-smith-admits-concern-over-links-with-heading-and-dementia> accessed 20 December 2020.
Simon Lloyd, ‘WAYNE ROONEY BACKS CALLS FOR INVESTIGATION INTO LINKS BETWEEN DEMENTIA AND HEADING’ (JOE) <https://www.joe.co.uk/sport/wayne-rooney-backs-calls-for-investigation-into-links-between-dementia-and-heading-256752> accessed 22 December 2020.
Richard Marsden and Mike Keegan, ‘David Beckham backs fight to tackle football dementia crisis: Former England captain says it is 'clear there are questions to be asked' about effects of heading ball’ (20 November 2020 Daily Mail) <https://www.dailymail.co.uk/news/article-8968611/David-Beckham-backs-fight-tackle-football-dementia-crisis.html> 20 December 2020.
MARTIN KEOWN, ‘As a player who headed the ball a lot in a professional career of more than 20 years, I’d be lying if I said I wasn’t concerned about my own long-term health’ (18 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8963831/MARTIN-KEOWN-Id-lying-said-wasnt-concerned-long-term-health.html> 20 December 2020.
Sam Blitz, ‘Joe Cole believes football is NOT doing enough and demands FA look into preventing dementia risk among players after Sir Bobby Charlton's shock diagnosis to follows deaths of England stars Nobby Stiles and Jack Charlton due to the illness’ (7 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/sportsnews/article-8924015/Joe-Cole-believes-football-NOT-doing-demands-FA-look-preventing-dementia-risk.html> accessed 20 December 2020.
PETER CROUCH ’I scored more headers than anyone so I know I'm at risk - that's why I'll have a dementia scan every year’ (23 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8979245/PETER-CROUCH-scored-headers-know-Im-risk.html> accessed 20 December 2020.
Danny Gallagher, ‘Gary Lineker calls for ban on HEADING in training at all levels, claiming “there is absolutely no reason” for it as research points to shocking increase in neurological diseases in former footballers’ (18 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8962461/Gary-Lineker-calls-ban-heading-training-levels.html> accessed 20 December 2020.
[27] Paul Gilmour and Husmukh Kerai, ‘Ryan Mason: Footballers guilty of being too brave over head injuries’ (1 December 2020 Sky News) <https://www.skysports.com/football/news/11095/12147135/ryan-mason-footballers-guilty-of-being-too-brave-over-head-injuries> accessed 2 December 2020.
[28] ‘PFA calls for “urgent intervention” to reduce and monitor heading in training’ (20 November 2020 The Guardian) <https://www.theguardian.com/football/2020/nov/20/pfa-calls-for-urgent-intervention-to-reduce-and-monitor-heading-in-training> accessed 20 December 2020.
[29] ‘Mike Bailey: Former Wolves captain diagnosed with dementia’ (27 November 2020 Sky News) <https://www.skysports.com/football/news/11699/12143806/mike-bailey-former-wolves-captain-diagnosed-with-dementia> accessed 20 December 2020.
‘Wolverhampton Wanderers: Former players association says dementia research is “long overdue”’(27 November 2020 BBC) <https://www.bbc.co.uk/sport/football/55102721> accessed 3 December 2020.
Patrick McPartlin, ‘Alex Cropley: Former Hibs, Arsenal, and Aston Villa midfielder diagnosed with dementia’ (10 December 2020 Edinburgh News) <https://www.edinburghnews.scotsman.com/sport/football/hibs/alex-cropley-former-hibs-arsenal-and-aston-villa-midfielder-diagnosed-dementia-3063467> accessed 20 December 2020.
‘Former England defender Kenny Sansom diagnosed with dementia’ (7 December 2020 The Athletic) <https://theathletic.com/news/kenny-sansom-dementia-latest/G57s5EqCNYYa> accessed 20 December 2020.
Matt Barlow, 'He loved heading, but it cost him everything... at the age of just 48 he’d forgotten how to sit down': Former Southampton star Kevin Moore died from dementia on his 55th birthday’ (22 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8975639/Heading-cost-Southampton-star-Kevin-Moore-died-dementia-55th-birthday.html> accessed 20 December 2020.
Mike Keegan, ‘“This job should carry a health warning”: The wife of former Arsenal and Tottenham defender Willie Young opens up about his fight with Alzheimer's and insists it was caused by “repetitive heading”’ <https://www.dailymail.co.uk/sport/football/article-9031433/The-wife-former-Arsenal-defender-Willie-Young-opens-fight-Alzheimers.html> accessed 20 December 2020.
Sachin Nakrani, ‘Football and dementia: players who died with or are living with the disease’ (3 November 2020 The Guardian) <https://www.theguardian.com/football/2020/nov/02/football-and-dementia-players-who-died-with-or-are-living-with-the-disease-england-1966> accessed 20 December 2020.
Andy Bull, ‘“Dementia in football is rife and the game is not doing enough to help”’ (2 November 2020 The Guardian) <https://www.theguardian.com/football/2020/nov/02/dementia-football-rife-game-not-doing-enough-to-help-chris-chilton-gary-chilton> accessed 20 November 2020.
Kieran Gill, ‘The forgotten England captain: Dave Watson won 65 caps for his country but has been let down by the PFA since his dementia diagnosis. Here, loving wife Penny reveals his heartbreaking story’ (6 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8922807/Dave-Watson-won-65-caps-England-let-PFA-dementia-diagnosis.html> accessed 20 November 2020.
Patrick Hill and Peter Robinson, ‘Brother of legendary goalie Peter Bonetti believes he developed Alzheimer's from heading heavy footballs’ (15 November 2020 Daily Record) <https://www.dailyrecord.co.uk/news/scottish-news/brother-peter-bonetti-believes-legendary-23010926> accessed 20 November 2020.
Charlie Walker, ‘PFA are still sweeping dementia in footballers “under the carpet” claims family of Wales international Alan Jarvis who died from Alzheimer's caused by the beautiful game, as son of Hull City striker Chris Chilton appeals for cash to pay care home bills’ (4 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8913267/PFA-sweeping-dementia-footballers-carpet-claims-family-Wales-international.html> accessed 20 November 2020.
[30] John Cross, ‘Geoff Hurst offers to donate brain for dementia research in tragic year for 1966 heroes’ (18 November 2020 Mirror) <https://www.mirror.co.uk/sport/football/news/sir-geoff-hurst-offers-donate-23026118> accessed 20 November 2020.
[31] Ian Herbert, ‘At least 500 former players are now affected by dementia with the PFA under fire for lack of help amid increased calls to investigate link between football and brain disease’ (14 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8949679/At-500-former-players-affected-dementia-PFA-fire.html> accessed 20 November 2020.
[32] Jack Rosser, ‘David Moyes calls on Nike and Adidas to create “heading ball” to decrease any brain damage to players’ (20 November 2020 Evening Standard) <https://www.standard.co.uk/sport/football/west-ham-david-moyes-nike-and-adidas-heading-ball-brain-damage-b74915.html> accessed 20 December 2020.
[33] Mike Keegan, ‘Enough is ENOUGH: Sportsmail launches campaign to tackle football's dementia scandal with a call for immediate action amid a growing number of former players affected by brain disease’ (16 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8955591/Enough-Sportsmail-launches-campaign-tackle-dementia.html> accessed 20 November 2020.
[34] Alistair Magowan, ‘Dementia in football: PFA to create taskforce to examine issue of brain injury diseases’ (18 November 2020 BBC) <https://www.bbc.co.uk/sport/football/54988097> accessed 20 December 2020.
[35] ‘Concussion substitute trials to begin from January’ (16 December 2020 BBC) <https://www.bbc.co.uk/sport/football/55335979> accessed 22 December 2020.
[36] Ian Herbert, ‘Battle to get brain injury among footballers recognised as an industrial disease - which would mean affected players being able to claim state disability benefits - is realistic, says expert’ (17 November 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-8959383/Industrial-disease-status-realistic-says-expert.html> accessed 20 November 2020.
[37] Ian Herbert, ‘Sportsmail's campaign to tackle dementia suffers setback as Industrial Injury Advisory Council requires more evidence in order to grant industrial disease designation’ (6 December 2020 Daily Mail) <https://www.dailymail.co.uk/sport/football/article-9024355/Setback-industrial-disease-designation-dementia-football.html> accessed 21 December 2020.
[38] Alistair Magowan, ‘Dementia in football: Former Premier League players join study’ (4 November 2020 BBC) <https://www.bbc.co.uk/sport/football/54799358> accessed 20 November 2020.
[39] ‘BIA-ALCL Physician Resources’ (15 December 2020 American Society of Plastic Surgeons) <https://www.plasticsurgery.org/for-medical-professionals/health-policy/bia-alcl-physician-resources> accessed 21 December 2020.
[40] ‘Symptoms of coronavirus’ (18 December 2020 NHS) <https://www.nhs.uk/conditions/coronavirus-covid-19/symptoms/> accessed 19 December 2020.
[41] Shivali Best, ‘New coronavirus symptom to look for as doctors warn rash in mouth could be sign’ (22 July 2020 The Mirror) <https://www.mirror.co.uk/science/new-coronavirus-symptom-look-doctors-22395319> accessed 22 July 2020.
Jimenez-Cauhe, Enanthem in Patients With COVID-19 and Skin Rash. JAMA Dermatology (2020) <https://jamanetwork.com/journals/jamadermatology/fullarticle/2768252> accessed 22 July 2020.
[42] Tim Spector, ‘Loss of smell and taste a key symptom for COVID-19 cases’ (1 April 2020 KCL) <https://www.kcl.ac.uk/news/loss-of-smell-and-taste-a-key-symptom-for-covid-19-cases> accessed 20 May 2020.
[43] ‘Six distinct “types” of COVID-19 identified’ (17 July 2020 King’s College London) <https://www.kcl.ac.uk/news/six-distinct-types-of-covid-19-identified> accessed 23 July 2020.
Sudre CH et al., Symptom clusters in Covid19: A potential clinical prediction tool from the COVID Symptom study app. MedRxiv 2020.06.12.20129056 https://www.medrxiv.org/content/10.1101/2020.06.12.20129056v1.full.pdf> accessed 23 July 2020.
[44] Meredith Wadman, Jennifer Couzin-Frankel, Jocelyn Kaiser and Catherine Matacic, ‘How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes’ (17 April 2020 Science Mag) <https://www.sciencemag.org/news/2020/04/how-does-coronavirus-kill-clinicians-trace-ferocious-rampage-through-body-brain-toes> accessed 20 December 2020.
[45] Ed Cara, ‘Kidneys, Brain, Skin: New Study Highlights the Whole-Body Damage Caused by Covid-19’ (21 July 2020 Gizmodo) <https://www.gizmodo.co.uk/2020/07/kidneys-brain-skin-new-study-highlights-the-whole-body-damage-caused-by-covid-19/> accessed 22 July 2020.
Gupta A et al., Extrapulmonary manifestations of COVID-19. Nature Medicine Volume 26, Pages 1017–1032(2020) <https://www.nature.com/articles/s41591-020-0968-3.pdf> accessed 22 July 2020.
[46] COVID-19 transmission—up in the air. Lancet Respiratory Medicine. VOLUME 8, ISSUE 12, P1159, DECEMBER 01, 2020 <https://www.thelancet.com/action/showPdf?pii=S2213-2600%2820%2930514-2> accessed 20 December 2020.
[47] ‘Coronavirus (COVID-19): What is social distancing?’ (4 March 2020 Public Health Matters) <https://publichealthmatters.blog.gov.uk/2020/03/04/coronavirus-covid-19-what-is-social-distancing/> accessed 18 December 2020.
[48] Public Health England, ‘Coronavirus (COVID-19): What is social distancing?’ (4 March 2020 GOV.UK) <https://publichealthmatters.blog.gov.uk/2020/03/04/coronavirus-covid-19-what-is-social-distancing/> accessed 9 March 2020.
[49] ‘Cases in United Kingdom’ (19 December 2020 GOV.UK) <https://coronavirus.data.gov.uk/details/cases> accessed 20 December 2020.
[50] ‘Deaths in United Kingdom’ (19 December 2020 GOV.UK) <https://coronavirus.data.gov.uk/details/deaths> accessed 20 December 2020.
[51] Sarah Caul, ‘Deaths registered weekly in England and Wales, provisional: week ending 4 December 2020’ (15 December 2020 ONS) <https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/weekending4december2020> accessed 29 December 2020.
[52] Government Office for Science and Scientific Advisory Group for Emergencies, ‘The R number and growth rate in the UK’ (18 December 2020 GOV.UK) <https://www.gov.uk/guidance/the-r-number-in-the-uk> accessed 20 December 2020.
[53] Vanessa Chalmers, ‘Professor Lockdown and team say Covid-19 kills 1.15% of all patients in wealthy countries like the UK due to our ageing population - FIVE TIMES as many as poorer countries with younger citizens’ (30 October 2020 Daily Mail) <https://www.dailymail.co.uk/news/article-8897015/Imperial-team-say-1-15-Covid-19-patients-die-despite-No10s-best-guess-0-5.html> accessed 20 December 2020.
Brazeau NF et al., Report 34: COVID-19 Infection Fatality Ratio: Estimates from Seroprevalence. Imperial
College London (29 October 2020 Imperial College London) <https://www.imperial.ac.uk/media/imperial-college/medicine/mrc-gida/2020-10-29-COVID19-Report-34.pdf> accessed 20 December 2020.
[54] ‘Are you immune to COVID-19? And could you catch it again? Here's what we know so far’ (12 October 2020 COVID Symptom Study) <https://covid.joinzoe.com/post/covid-reinfection-immunity> accessed 20 December 2020.
[55] Long QX et al., Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med (2020) <https://www.nature.com/articles/s41591-020-0965-6.pdf> accessed 26 June 2020.
Seow J et al., Longitudinal evaluation and decline of antibody responses in SARS-CoV-2 infection. medRxiv 2020.07.09.20148429. <https://www.medrxiv.org/content/10.1101/2020.07.09.20148429v1.full.pdf> accessed20 December 2020.
[56] Medicines and Healthcare products Regulatory Agency, ‘UK medicines regulator gives approval for first UK COVID-19 vaccine’ (2 December 2020 GOV.UK) <https://www.gov.uk/government/news/uk-medicines-regulator-gives-approval-for-first-uk-covid-19-vaccine> accessed 20 December 2020.
[57] ‘PFIZER AND BIONTECH CONCLUDE PHASE 3 STUDY OF COVID-19 VACCINE CANDIDATE, MEETING ALL PRIMARY EFFICACY ENDPOINTS’ (18 November 2020 Pfizer) <https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine> accessed 20 December 2020.
[58] Department of Health and Social Care, ‘More than 137,000 people in UK receive first dose of COVID vaccine in one week’ (16 December 2020 GOV.UK) <https://www.gov.uk/government/news/more-than-137000-people-in-uk-receive-first-dose-of-covid-vaccine-in-one-week> accessed 20 December 2020.
[59] Molly Blackall and Denis Campbell, ‘Oxford vaccine still under review, says UK medicine agency’ (19 December 2020 The Guardian) <https://www.theguardian.com/world/2020/dec/19/oxford-vaccine-still-under-review-says-uk-medicine-agency> accessed 20 December 2020.
[60] Niko Kommenda and Frank Hulley-Jones, ‘Covid vaccine tracker: when will a coronavirus vaccine be ready?’ (10 November 2020 The Guardian) https://www.theguardian.com/world/ng-interactive/2020/nov/10/covid-vaccine-tracker-when-will-a-coronavirus-vaccine-be-ready> accessed 20 December 2020.
[61] Samuel Lovett, ‘New coronavirus strain up to 70% more transmissible, government says’ (20 December 2020 The Independent) <https://www.independent.co.uk/news/health/coronavirus-strain-covid-transmission-b1776581.html> accessed 21 December 2020.
[62] ‘Is the vaccine effective against the new coronavirus strain? Everything you need to know’ (15 December 2020 The Independent) <https://www.independent.co.uk/news/health/covid-uk-new-strain-mutation-b1773908.html> accessed 20 December 2020.
[63] Dr. Ben Windsor-Shellard and Jasveer Kaur, ‘Coronavirus (COVID-19) related deaths by occupation, England and Wales: deaths registered between 9 March and 25 May 2020’ (26 June 2020 ONS) <https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/bulletins/coronaviruscovid19relateddeathsbyoccupationenglandandwales/deathsregisteredbetween9marchand25may2020> accessed 1 July 2020.
[64] Table 1 of ONS dataset.
[65] Sam Corbishley, ‘Health workers still three times more likely to catch coronavirus despite PPE’ (1 August 2020 Metro) <https://metro.co.uk/2020/08/01/health-workers-still-three-times-likely-catch-coronavirus-despite-ppe-13068209/> accessed 6 August 2020.
Nguyen LH et al., Risk of COVID-19 among front-line health-care workers and the general community: a prospective cohort study. Lancet Public Health (2020) <https://www.thelancet.com/action/showPdf?pii=S2468-2667%2820%2930164-X> accessed 6 August 2020.
Becky Tinsley, ‘Impact of coronavirus in care homes in England: 26 May to 19 June 2020’ (3 July 2020 ONS) <https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/impactofcoronavirusincarehomesinenglandvivaldi/26mayto19june2020> accessed 15 July 2020.
Vanessa Chalmers, ‘NHS hospital in Bristol discharged 213 untested patients and 20 who had previously been diagnosed with Covid-19 into care homes, investigation reveals’ (10 July 2020 The Daily Mail) <https://www.dailymail.co.uk/news/article-8510031/NHS-hospital-Bristol-discharged-213-untested-patients-20-Covid-19-care-homes.html> accessed 15 July 2020.
‘Coronavirus: Hinckley care home staff “did not always wear masks”’ (10 August 2020 BBC) <https://www.bbc.co.uk/news/uk-england-leicestershire-53722450> accessed 11 August 2020.
[66] Sarah Boseley and Aamna Mohdin, ‘Daughter urges inquiry into Covid-19 deaths of bus drivers in England’ (27 July 2020 The Guardian) <https://www.theguardian.com/world/2020/jul/27/earlier-lockdown-could-have-saved-lives-of-london-bus-drivers-says-report-coronavirus> accessed 6 August 2020.
Emma Bartholomew, ‘Coronavirus: ‘Fewer London bus drivers would have died had lockdown come sooner’, UCL report finds’ (28 July 2020 Islington Gazette) <https://www.islingtongazette.co.uk/news/fewer-bus-drivers-would-have-died-if-lockdown-had-come-sooner-1-6767238> accessed 6 August 2020.
Nigel Barlow, ‘Study reveals COVID-19 transmission rate on trains’ (3 August 2020 About Manchester) <https://aboutmanchester.co.uk/study-reveals-covid-19-transmission-rate-on-trains/> accessed 6 August 2020.
Hu M et al., The risk of COVID-19 transmission in train passengers: an epidemiological and modelling study. Clinical Infectious Diseases, ciaa1057. <https://academic.oup.com/cid/article-pdf/doi/10.1093/cid/ciaa1057/33543762/ciaa1057.pdf> accessed 6 August 2020.
[67] Natasha Lomas, ‘Deliveroo criticized over ‘inadequate’ PPE provision and income support for riders risking coronavirus exposure’ (13 May 2020 Tech Crunch) <https://techcrunch.com/2020/05/13/deliveroo-criticized-over-inadequate-ppe-provision-and-income-support-for-riders-risking-coronavirus-exposure/> accessed 18 May 2020.
Ashleigh Webber, ‘Denying toilet access “a serious public health matter", warns union’ (17 June 2020 Personnel Today) <https://www.personneltoday.com/hr/denying-toilet-access-a-serious-public-health-matter/> accessed 8 July 2020.
[68] ‘Coronavirus: DPD parcel delivery firm staff in Oldbury test positive’ (15 August 2020 BBC) <https://www.bbc.co.uk/news/uk-england-birmingham-53790764> accessed 20 August 2020.
[69] Kevin White, ‘Trade unions slam rocketing number of Covid-19 cases at UK food manufacturing plants’ (2 July 2020 The Grocer) <https://www.thegrocer.co.uk/meat/trade-unions-slam-rocketing-number-of-covid-19-cases-at-uk-food-manufacturing-plants/646027.article> accessed 7 July 2020.
Chris Jewers and Luke May, ‘Staff at coronavirus-hit food factory run by firm that supplies Sainsbury's and Asda say they begged bosses to shut it down after 237 workers tested positive for Covid-19’ (30 June 2020 The Daily Mail) <https://www.dailymail.co.uk/news/article-8476223/Staff-coronavirus-hit-food-factory-say-begged-bosses-shut-down.html> accessed 15 July 2020.
‘Coronavirus: Third West Yorkshire bed factory outbreak’ (13 July 2020 BBC) <https://www.bbc.co.uk/news/uk-england-leeds-53394717> accessed 14 July 2020.
‘Outbreak of Covid-19 at Alconbury flower and fruit distributor’ (20 July 2020 BBC) <https://www.bbc.co.uk/news/uk-england-cambridgeshire-53451100> accessed 22 July 2020.
Greg Heffer, ‘Coronavirus: “Significant concerns” about Leicester clothing factories, says Matt Hancock’ <https://news.sky.com/story/coronavirus-significant-concerns-about-leicester-clothing-factories-says-matt-hancock-12021655> accessed 7 July 2020.
[70] ‘RIDDOR reporting of COVID-19’ (1 December 2020 HSE) <https://www.hse.gov.uk/coronavirus/riddor/index.htm> accessed 21 December 2020.
[71] ‘Management information: Coronavirus (COVID-19) disease reports’ (HSE) <https://www.hse.gov.uk/statistics/coronavirus/index.htm> accessed 21 December 2020.
[72] ‘Epidemic of pandemic claims yet to materialise’ (3 August 2020 Law Gazette) <https://www.lawgazette.co.uk/obiter/epidemic-of-pandemic-claims-yet-to-materialise/5105192.article> accessed 5 August 2020.
[73] Neil Rose, ‘Covid-related PI claims “gaining momentum”, warns defendant firm’ (17 December 2020 Litigation Futures) <https://www.litigationfutures.com/news/covid-related-claims-gaining-momentum-warns-defendant-firm> accessed 20 December 2020.
[74] Chris Stubbs and Martin Stockdale, ‘COVID-19 claims farming, risk level: high’ (6 May 2020 Kennedys) <https://www.kennedyslaw.com/thought-leadership/blogs/fraud-blog-fundamentally-honest/covid-19-claims-farming-risk-level-high-1/> accessed 12 May 2020.
[75] The Management of Health & Safety at Work Regulations (MHSWR) 1999
Manual Handling Operations Regulations (MHO) 1992
Display Screen Equipment Regulations (DSE) 1992
Workplace (Health, Safety and Welfare) Regulations (WHSW) 1992
Provision and use of Work Equipment Regulations (PUWER) 1992
Personal Protective Equipment (PPE) at Work Regulations 1992
The Control of Substances Hazardous to Health Regulations 2002 (as amended)
[76] Marcus Grant, ‘S. 69 Enterprise and Regulatory Reform Act 2013 “Where are we, 5½ years on?”’ (23 March 2019 Temple Garden Chambers) <https://tgchambers.com/wp-content/uploads/2019/03/MGs-PIBA-2019-Talk_FINAL.pdf> accessed 19 May 2020.
[77] Government Office for Science and Scientific Advisory Group for Emergencies, ‘Coronavirus (COVID-19): scientific evidence supporting the UK government response’ (5 August 2020 GOV.UK) <https://www.gov.uk/government/news/coronavirus-covid-19-scientific-evidence-supporting-the-uk-government-response> accessed 5 July 2020.
[78] Employers could face legal action over COVID-19 exposure, expert warns’ (1 June 2020 University of Stirling) <https://www.stir.ac.uk/news/2020/june-2020-news/employers-could-face-legal-action-over-covid-19-exposure-expert-warns/> accessed 6 June 2020.
Watterson A, COVID-19 in the UK and Occupational Health and Safety: Predictable not Inevitable Failures by Government, and Trade Union and Nongovernmental Organization Responses. NEW SOLUTIONS: A Journal of Environmental and Occupational Health Policy 0(0) 1–9 (2020) <https://journals.sagepub.com/doi/10.1177/1048291120929763> accessed 6 June 2020.
[79] Memoli MJ et al., Validation of the Wild-type Influenza A Human Challenge Model H1N1pdMIST: An A(H1N1)pdm09 Dose-Finding Investigational New Drug Study. Clin Infect Dis. 2015 Mar 1; 60(5): 693–702. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4342672/pdf/ciu924.pdf> accessed 24 June 2020.
[80] Chu CM et al., Viral Load Distribution in SARS Outbreak. Emerging Infectious Diseases Vol. 11, No. 12, December 2005 <https://wwwnc.cdc.gov/eid/article/11/12/pdfs/04-0949.pdf> accessed 6 July 2020.
Hung IFN et al., Viral loads in clinical specimens and SARS manifestations. Hong Kong Med J 2009;15(Suppl 9):S20-2. <https://www.hkmj.org/system/files/hkm0912sp9p20.pdf> accessed 6 July 2020.
[81] Sarah Caddy, ‘Coronavirus: does the amount of virus you are exposed to determine how sick you’ll get’ (7 April 2020 The Conversation) <https://theconversation.com/coronavirus-does-the-amount-of-virus-you-are-exposed-to-determine-how-sick-youll-get-135119> accessed
[82] Andrew Morgan and Richard Kenyon, ‘Bringing a civil claim following death or injury from Covid-19’ (15 May 2020 HR News) <http://hrnews.co.uk/bringing-a-civil-claim-following-death-or-injury-from-covid-19/> accessed 22 May 2020.
[83] Sarah Newey, ‘Revealed: How coronavirus attacks your veins, heart, brain and blood – as well as lungs’ (24 April 2020 The Telegraph) <https://www.telegraph.co.uk/global-health/science-and-disease/revealed-coronavirus-attacks-veins-heart-brain-blood-lungs/> accessed 22 May 2020.
Stuart Ramsay, ‘Coronavirus warning from Italy: Effects of COVID-19 could be worse than first thought’ (13 July 2020 Sky News) <https://news.sky.com/story/coronavirus-warning-from-italy-effects-of-covid-19-could-be-worse-than-first-thought-12027348> accessed 13 July 2020.
[84] Ian Randall, ‘Coronavirus “harms the brain and nervous system of HALF of severely ill patients and a third of all cases” — causing symptoms such as stumbling, slurred speech and seizures’ (10 April 2020 The Daily Mail) <https://www.dailymail.co.uk/sciencetech/article-8208417/In-half-severe-cases-COVID-19-affect-brain-nervous-too.html> accessed 17 July 2020.
Mao L et al., Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683-690 <https://jamanetwork.com/journals/jamaneurology/fullarticle/2764549> accessed 17 July 2020.
[85] Shannon Halloway and Bryan D. James, ‘A Tsunami of Dementia Could Be on the Way’ (19 May 2020 The Scientific American) <https://blogs.scientificamerican.com/observations/a-tsunami-of-dementia-could-be-on-the-way/> accessed 22 May 2020.
Jeremy Rossman, ‘Coronavirus: many patients reporting neurological symptoms’ (24 April 2020 The Conversation) <https://theconversation.com/coronavirus-many-patients-reporting-neurological-symptoms-136692> accessed 22 May 2020.
Hannah Paine, ‘Coronavirus: UK research reveals COVID-19 could cause Alzheimer’s, lung damage and psychological trauma’ (23 June 2020 News.com.au) <https://www.news.com.au/lifestyle/health/health-problems/coronavirus-uk-research-reveals-covid19-could-cause-alzheimers-lung-damage-and-psychological-trauma/news-story/092667263cb54df90778c4c36489f4b7> accessed 30 June 2020.
Helms J et al., Neurologic Features in Severe SARS-CoV-2 Infection. N Engl J Med 2020; 382:2268-2270. https://www.nejm.org/doi/pdf/10.1056/NEJMc2008597?articleTools=true> accessed 5 June 2020.
Kanberg N et al., Neurochemical evidence of astrocytic and neuronal injury commonly found in COVID-19. Neurology (2020) <https://n.neurology.org/content/neurology/early/2020/06/16/WNL.0000000000010111.full.pdf> accessed 30 June 2020.
Varatharaj A et al., Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. Lancet (2020) <https://www.thelancet.com/action/showPdf?pii=S2215-0366%2820%2930287-X> accessed 2 July 2020.
Jack Rear, ‘Is delirium another complication of Covid-19?’ (28 July 2020 The Telegraph) <https://www.telegraph.co.uk/health-fitness/mind/delirium-another-complication-covid-19/> accessed 3 August 2020.
Joe Pinkstone, ‘More than HALF of hospitalised Covid-19 patients develop a psychiatric disorder after being discharged, Italian study finds’ (3 August 2020 Daily Mail) <https://www.dailymail.co.uk/sciencetech/article-8588693/Some-COVID-19-survivors-suffer-psychiatric-disorders-Italian-study-says.html> accessed 4 August 2020.
Mazza MG et al., Anxiety and depression in COVID-19 survivors: role of inflammatory and clinical predictors. Brain, Behavior and Immunity (2020) <https://www.sciencedirect.com/science/article/pii/S0889159120316068/pdfft?md5=b0327d189ae7ff62d881c556232151ff&pid=1-s2.0-S0889159120316068-main.pdf> accessed 4 August 2020.
Professor Natalie Tronson, ‘How COVID-19 might increase risk of memory loss and cognitive decline’ (7 August 2020 The Conversation) <https://theconversation.com/how-covid-19-might-increase-risk-of-memory-loss-and-cognitive-decline-141940> accessed 10 August 2020.
Cohen ME et al., A case of probable Parkinson's disease after SARS-CoV-2 infection. Lancet Neurology. VOLUME 19, ISSUE 10, P804-805, OCTOBER 01, 2020 <https://www.thelancet.com/action/showPdf?pii=S1474-4422%2820%2930305-7> accessed 17 December 2020.
[86] ‘COVID-19 is making tinnitus worse – new study’ (6 November 2020 BSA) <https://www.thebsa.org.uk/covid-19-is-making-tinnitus-worse-new-study/> accessed 23 December 2020.
[87] Fergus Walsh, ‘Coronavirus: What does Covid-19 do to the brain?’ (1 July 2020 BBC) <https://www.bbc.co.uk/news/health-53081022> accessed 2 July 2020.
[88] Mary Kekatos, ‘Coronavirus patients are EIGHT TIMES more likely to suffer a stroke than flu patients, study finds’ (2 July 2020 The Daily Mail) <https://www.dailymail.co.uk/health/article-8483603/Coronavirus-patients-eight-times-likely-suffer-stroke-compared-flu-patients.html> accessed 3 July 2020.
Merkler AE et al., Risk of Ischemic Stroke in Patients With Coronavirus Disease 2019 (COVID-19) vs Patients With Influenza. JAMA Neurol (2020) <https://jamanetwork.com/journals/jamaneurology/fullarticle/2768098> accessed 3 July 2020.
[89] Oxley TJ., Large-Vessel Stroke as a Presenting Feature of Covid-19 in the Young. N Engl J Med. 2020 May 14;382(20):e60. <https://www.nejm.org/doi/pdf/10.1056/NEJMc2009787?articleTools=true> accessed 5 June 2020.
Berekashvili K et al., Etiologic Subtypes of Ischemic Stroke in SARS-COV-2 Virus patients in a cohort of New York City hospitals. MedRxiv 2020.05.03.20077206 <https://www.medrxiv.org/content/10.1101/2020.05.03.20077206v2.full.pdf> accessed 5 June 2020.
[90] Sarah Boseley, ‘Why doctors say UK is better prepared for a second wave of coronavirus’ (22 June 2020 The Guardian) <https://www.theguardian.com/world/2020/jun/22/why-doctors-say-uk-better-prepared-for-second-wave-coronavirus> accessed 22 June 2020.
Ackermann M et al., Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Engl J Med. 2020 May 21. <https://www.nejm.org/doi/pdf/10.1056/NEJMoa2015432> accessed 22 June 2020.
[91]Barco S et al., Incomplete echocardiographic recovery at 6 months predicts long-term sequelae after intermediate-risk pulmonary embolism. A post-hoc analysis of the Pulmonary Embolism Thrombolysis (PEITHO) trial. Clinical Research in Cardiology; Volume 108, pages 772–778(2019) <https://link.springer.com/content/pdf/10.1007/s00392-018-1405-1.pdf> accessed 5 June 2020.
Chris Morris, ‘Coronavirus: 'Baffling' observations from the front line’ (23 May 2020 BBC) <https://www.bbc.co.uk/news/52760992> accessed 5 June 2020.
[92] ‘Advisory Board: its not just lungs: COVID-19 may damage the heart, brain and kidneys’ (17 April 2020 Advisory Board). <https://www.advisory.com/daily-briefing/2020/04/17/organ-damage> accessed 5 June 2020.
[93] Jane Kirby, ‘Severe Covid-19 illness “can damage” the heart’ (13 July 2020 Belfast Telegraph) <https://www.belfasttelegraph.co.uk/news/health/coronavirus/severe-covid-19-illness-can-damage-the-heart-39361657.html> accessed 13 July 2020.
Dweck MR et al., Global evaluation of echocardiography in patients with COVID-19. European Heart Journal - Cardiovascular Imaging, jeaa178, <https://academic.oup.com/ehjcimaging/article-pdf/doi/10.1093/ehjci/jeaa178/33402488/jeaa178.pdf> accessed 13 July 2020.
[94] Will Bedingfield, ‘How coronavirus destroys the human body, one organ at a time’ (19 May 2020 WIRED) <https://www.wired.co.uk/article/how-coronavirus-kills> accessed 22 May 2020.
Lucy Jones, ‘LASTING DAMAGE The long-term effects of coronavirus on the body – from lung scarring to liver damage’ (22 April 2020 The Sun) <https://www.thesun.co.uk/news/11455834/long-term-effects-coronavirus-body/> accessed 22 May 2020.
Huang C et al., Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020 Feb 15;395(10223):497-506. <https://www.thelancet.com/action/showPdf?pii=S0140-6736%2820%2930183-5> accessed 3 June 2020.
Madjid M et al., Potential Effects of Coronaviruses on the Cardiovascular System. JAMA Cardiol. Published online March 27, 2020. <https://jamanetwork.com/journals/jamacardiology/fullarticle/2763846> accessed 5 June 2020.
Zheng YY et al., COVID-19 and the cardiovascular system. Nature Reviews Cardiology. Volume 17, Pages 259–260(2020). <https://www.nature.com/articles/s41569-020-0360-5.pdf> accessed 5 June 2020.
Shi S et al., Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020 Mar 25;e200950. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7097841/> accessed 5 June 2020.
[95] Ahmed MZ et al., Thrombocytopenia as an Initial Manifestation of COVID-19; Case Series and Literature Review. Br J Haematol. 2020 May 5. <https://onlinelibrary.wiley.com/doi/epdf/10.1111/bjh.16769> accessed 5 June 2020.
[96] Georgia Arlott, Coronavirus: Thousands of COVID-19 survivors could be diagnosed with sepsis, charity warns’ (28 July 2020 Sky News) <https://news.sky.com/story/coronavirus-thousands-of-covid-19-survivors-could-be-diagnosed-with-sepsis-charity-warns-12037944> accessed 29 July 2020.
‘NEW DATA HIGHLIGHT THE RISK OF REPEAT INFECTIONS IN COVID-19 SURVIVORS’ (THE UK SEPSIS TRUST) <https://sepsistrust.org/new-data-highlight-the-risk-of-repeat-infections-in-covid-19-survivors/> accessed 5 August 2020.
[97] Laura Donnelly, ‘Revealed: Scars of Covid-19 could last for life as doctors warn of long-term damage to health’ (22 June 2020 The Telegraph) <https://www.telegraph.co.uk/news/2020/06/22/revealed-scars-covid-19-could-last-life-doctors-warn-long-term/?utm_content=telegraph&utm_medium=Social&utm_campaign=Echobox&utm_source=Twitter#Echobox=1592897602> accessed 30 June 2020.
Shi H et al., Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis. 2020 Apr;20(4):425-434. <https://www.thelancet.com/action/showPdf?pii=S1473-3099%2820%2930086-4> accessed 3 June 2020.
Wang Y et al., Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology. 2020 Mar 19;200843. <https://pubs.rsna.org/doi/pdf/10.1148/radiol.2020200843> accessed 3 June 2020.
[98] ‘Coronavirus: Warning thousands could be left with lung damage’ (23 June 2020 BBC) 2 July 2020 <https://www.bbc.co.uk/news/health-53065340> accessed 2 July 2020.
[99] Wu D et al., Plasma Metabolomic and Lipidomic Alterations Associated with COVID-19. <https://www.medrxiv.org/content/10.1101/2020.04.05.20053819v3.full.pdf> accessed 22 May 2020.
Zhang et al., Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. 2020 May;5(5):428-430. <https://www.thelancet.com/action/showPdf?pii=S2468-1253%2820%2930057-1> accessed 3 June 2020.
[100] Meredith Wadman et al., ‘How does coronavirus kill? Clinicians trace a ferocious rampage through the body, from brain to toes’ (17 April 2020 Science Mag) <https://www.sciencemag.org/news/2020/04/how-does-coronavirus-kill-clinicians-trace-ferocious-rampage-through-body-brain-toes> accessed 22 May 2020.
[101] Lucy Jones, ‘NEW SIGN Neck pain could be a sign of rare complication of coronavirus, docs discover’ (21 May 2020 The Sun) <https://www.thesun.co.uk/news/11675359/neck-pain-sign-rare-complication-coronavirus/> accessed 22 May 2020.
[102] Dr. John Sperati, ‘Coronavirus: Kidney Damage Caused by COVID-19’ (14 May 2020 John Hopkins Medicine) <https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-kidney-damage-caused-by-covid19> accessed 14 July 2020.
[103] Hirsch JS et al., Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020 May 13;S0085-2538(20)30532-9. <https://www.kidney-international.org/article/S0085-2538(20)30532-9/pdf> accessed 22 May 2020.
[104] Bornstein SR et al., Practical recommendations for the management of diabetes in patients with COVID-19. Lancet. Volume 8, Issue 6, June 2020, Pages 546-550 <https://www.sciencedirect.com/science/article/pii/S2213858720301522/pdfft?md5=d24aa8e38368f0ecb1a9ca03530d5636&pid=1-s2.0-S2213858720301522-main.pdf> accessed 30 June 2020.
Rubino F et al., New-Onset Diabetes in Covid-19. N Engl J Med (2020) <https://www.nejm.org/doi/pdf/10.1056/NEJMc2018688?articleTools=true> accessed 30 June 2020.
[105] Sarah Newey, ‘Covid-19 may trigger diabetes, growing body of evidence suggests’ (25 June 2020 The Telegraph) <https://www.telegraph.co.uk/global-health/science-and-disease/covid-19-may-trigger-diabetes-growing-body-evidence-suggests/> accessed 30 June 2020.
Jessica Carpani, ‘Covid-19 may trigger the onset of diabetes in previously healthy people’ (12 June 2020 The Telegraph) <https://www.telegraph.co.uk/news/2020/06/12/covid-19-may-trigger-onset-diabetes-previously-healthy-people/> accessed 30 June 2020.
Maxine Myers, ‘COVID-19 linked to increase in type 1 diabetes in children’ (18 August 2020 Imperial College London) <https://www.imperial.ac.uk/news/201473/covid-19-linked-increase-type-diabetes-children/> accessed 20 August 2020.
Unsworth R et al., New-Onset Type 1 Diabetes in Children During COVID-19: Multicenter Regional Findings in the U.K. Diabetes Care 2020 Aug; dc201551. <https://care.diabetesjournals.org/content/early/2020/08/13/dc20-1551.full-text.pdf> accessed 20 August 2020.
[106] Priya Hays, Clinical sequelae of the novel coronavirus: does COVID-19 infection predispose patients to cancer? Future Medicine. (27 May 2020) <https://www.futuremedicine.com/doi/pdf/10.2217/fon-2020-0300> accessed 5 June 2020.
[107] Abobaker A and Raba AA, Does COVID-19 affect male fertility? World J Urol. 2020 Apr 21 : 1–2. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7171435/pdf/345_2020_Article_3208.pdf> accessed 5 June 2020.
[108] Li D et al., Clinical Characteristics and Results of Semen Tests Among Men With Coronavirus Disease 2019. JAMA Netw Open. 2020 May 1;3(5):e208292. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7206502/> accessed 5 June 2020.
Ma L et al., Effect of SARS-CoV-2 infection upon male gonadal function: A single center-based study. MedRxiv 2020.03.21.20037267. <https://www.medrxiv.org/content/10.1101/2020.03.21.20037267v2.full.pdf> accessed 5 June 2020.
[109] Katrina Turrill, ‘Coronavirus update: The sign in a person’s hair that could signal COVID-19’ (8 August 2020 The Express) https://www.express.co.uk/life-style/health/1320412/coronavirus-update-cases-symptoms-hair-loss-covid-19> accessed 11 August 2020.
Rivetti N and Baruscotti S, Management of telogen effluvium during the COVID‐19 emergency: Psychological implications. Dermatologic Therapy (2020) <https://onlinelibrary.wiley.com/doi/epdf/10.1111/dth.13648> accessed 11 August 2020.
Emma Brazell, ‘Hair loss may be long-term side effect from coronavirus’ (6 August 2020 Metro) <https://metro.co.uk/2020/08/06/hair-loss-may-long-term-side-effect-coronavirus-13091035/> accessed 11 August 2020.
[110] Riphagen S et al., Hyperinflammatory shock in children during COVID-19 pandemic. Lancet. 2020 23-29 May; 395(10237): 1607–1608. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7204765/pdf/main.pdf> accessed 5 June 2020.
Feldstein LR et al., Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med (2020) <https://www.nejm.org/doi/pdf/10.1056/NEJMoa2021680?articleTools=true> accesse 30 June 2020.
Dufort EM et al., Multisystem Inflammatory Syndrome in Children in New York State. N Engl J Med (2020) <https://www.nejm.org/doi/pdf/10.1056/NEJMoa2021756?articleTools=true> accessed 30 June 2020.
Vishwadha Chander, ‘Rare syndrome linked to COVID-19 found in nearly 600 U.S. children -CDC’ (7 August 2020 Reuters) <https://uk.reuters.com/article/uk-health-coronavirus-children/rare-syndrome-linked-to-covid-19-found-in-nearly-600-u-s-children-cdc-idUKKCN25335V> accessed 10 August 2020.
[111] Toubiana J et al., Kawasaki-like multisystem inflammatory syndrome in children during the covid-19 pandemic in Paris, France: prospective observational study. BMJ. 2020; 369 :m2094 https://www.bmj.com/content/369/bmj.m2094.full.pdf> accessed 5 June 2020.
Imogen Braddick, ‘Rare syndrome linked to Covid-19 “affects children with African heritage more”’ (3 June 2020 The Evening Standard) <https://www.standard.co.uk/news/health/coronavirus-syndrome-children-kawasaki-disease-african-a4459176.html#gsc.tab=0> accessed 5 June 2020.
[112] Vanessa Chalmers, ‘At least TWO British children have died from mysterious Kawasaki-like disease linked to Covid-19, study reveals’ (10 July 2020 The Daily Mail) <https://www.dailymail.co.uk/news/article-8509473/Two-children-die-Kawasaki-like-disease-linked-Covid-19-study-78-British-children.html> accessed 13 July 2020.
Davies P et al., Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health (2020) <https://www.thelancet.com/action/showPdf?pii=S2352-4642%2820%2930215-7> accessed 13 July 2020.
[113] ‘Coronavirus-related children's diseases linked to blood cell changes – study’ (10 August 2020 University of Birmingham) <https://www.birmingham.ac.uk/news/latest/2020/08/children's-diseases-linked-to-blood-cell-changes.aspx> accessed 10 August 2020.
Syrimi E et al., Single-cell RNA-seq reveals profound monocyte changes in Paediatric Inflammatory Multisystem Syndrome Temporally associated with SARS-CoV-2 infection (PIMS-TS). MedRxiv 2020.08.06.20164848; https://www.medrxiv.org/content/10.1101/2020.08.06.20164848v1.full.pdf> accessed 10 August 2020.
[114] Matt Mathers, ‘Coronavirus tips: How worried should pregnant women be about coronavirus?’ (11 May 2020 The Independent) <https://www.independent.co.uk/life-style/health-and-families/coronavirus-pregnant-women-birth-baby-risk-covid-19-a9390131.html> accessed 22 May 2020.
Connor Boyd, ‘Mothers with Covid-19 are 'unlikely' to infect their babies during breastfeeding as long as they wear masks and practise good hygiene, study finds’ (24 July 2020 Daily Mail) <https://www.dailymail.co.uk/news/article-8555877/Mothers-Covid-19-unlikely-infect-babies-breastfeeding.html> accessed 6 August 2020.
Francesco Guarascio, ‘WHO urges mothers to breastfeed even if infected with COVID-19’ (3 August 2020 Reuters) <https://uk.reuters.com/article/us-health-coronavirus-who-breastfeeding/who-urges-mothers-to-breastfeed-even-if-infected-with-covid-19-idUKKBN24Z1B7> accessed 3 August 2020.
[115] Ross Lydall, ‘Doctors begin study into effects of coronavirus on pregnant women’ (11 August 2020 Evening Standard) <https://www.standard.co.uk/news/health/study-risks-coronavirus-pregnancy-a4521751.html> accessed 11 August 2020.
[116] Nina Massey and Brett Gibbons, ‘Embryos vulnerable to Covid-19 infection from second week of pregnancy, study shows’ (5 August 2020 Wales Online) <https://www.walesonline.co.uk/news/uk-news/embryos-vulnerable-covid-19-infection-18716876> accessed 5 August 2020.
‘Study suggests embryos could be susceptible to coronavirus as early as second week of pregnancy’ (5 August 2020 University of Cambridge) <https://www.cam.ac.uk/research/news/study-suggests-embryos-could-be-susceptible-to-coronavirus-as-early-as-second-week-of-pregnancy> accessed 5 August 2020.
Weatherbee BAT et al., Expression of SARS-CoV-2 receptor ACE2 and the protease TMPRSS2 suggests susceptibility of the human embryo in the first trimester. Open Biology Volume 10 Issue 8 (2020) <https://royalsocietypublishing.org/doi/pdf/10.1098/rsob.200162> accessed 5 August 2020.
[117] Gerrard Kaonga, ‘Matt Hancock “concerned” about devastating “long-term” impacts of COVID-19’ (The Express) <https://www.express.co.uk/news/uk/1309743/Matt-Hancock-coronavirus-news-latest-long-term-impact-update-COVID-19> accessed 16 July 2020.
[118] ‘Coronavirus: Calls for awareness of long-term effects’ (19 June 2020 BBC) <https://www.bbc.co.uk/news/uk-england-south-yorkshire-53084368> accessed 23 June 2020.
Laura Sharman, Laura Sharman and Stephanie Balloo, ‘Coronavirus survivor still feels like she's "been hit by a truck" 100 days on’ (19 July 2020 The Mirror) <https://www.mirror.co.uk/news/uk-news/covid-survivors-still-suffer-symptoms-22379782> accessed 19 July 2020.
Jackson Barron and Zoe Zaczek, ‘COVID-19 survivors say they are suffering horrific symptoms MONTHS after being cleared of the virus - as experts warn “we don't know the long-term effects”’ (27 July 2020 Daily Mail) <https://www.dailymail.co.uk/news/article-8561267/COVID-19-survivors-reveal-suffering-symptoms-virus-MONTHS-left-bodies.html> accessed 7 August 2020.
Lara Keay, ‘Long-term COVID warning: ICU doctor reports having coronavirus symptoms for three months’ (25 June 2020 Sky News) <https://news.sky.com/story/long-term-covid-warning-icu-doctor-reports-having-coronavirus-symptoms-for-three-months-12014361> accessed 30 June 2020.
[119] ‘One in 20 people likely to suffer from “Long COVID”, but who are they?’ (21 October 2020 COVID Symptom Study) <https://covid.joinzoe.com/post/long-covid> accessed 17 December 2020.
Sudre CH et al., Attributes and predictors of Long-COVID: analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App. medRxiv 2020.10.19.20214494; <https://www.medrxiv.org/content/10.1101/2020.10.19.20214494v1.full.pdf> accessed 20 December 2020.
[120] Department of Health and Social Care and The Rt Hon Matt Hancock MP, ‘Research study into long-term health impacts of COVID-19 launched in the UK’ (7 August 2020 GOV.UK) <https://www.gov.uk/government/news/research-study-into-long-term-health-impacts-of-covid-19-launched-in-the-uk> accessed 11 August 2020.
[121] Nicola Davis, ‘Participants in UK coronavirus study could be monitored for up to 25 years’ (10 July 2020 The Guardian) <https://www.theguardian.com/world/2020/jul/10/participants-uk-coronavirus-study-could-be-monitored-25-years> accessed 13 July 2020.
[122] ‘Coronavirus: NHS England launches tool to aid long-term recovery’ (5 July 2020 BBC) <https://www.bbc.co.uk/news/health-53291925> accessed 7 July 2020.
[123] Petersen I and Phillips A, Three Quarters of People with SARS-CoV-2 Infection are Asymptomatic: Analysis of English Household Survey Data. Clin Epidemiol. 2020;12:1039-1043 <https://www.dovepress.com/three-quarters-of-people-with-sars-cov-2-infection-are-asymptomatic-an-peer-reviewed-fulltext-article-CLEP> accessed 17 December 2020.
[124] Ian Sample, ‘Warning of serious brain disorders in people with mild coronavirus symptoms’ (8 July 2020 The Guardian) <https://www.theguardian.com/world/2020/jul/08/warning-of-serious-brain-disorders-in-people-with-mild-covid-symptoms> accessed 17 July 2020.
Paterson RW, The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain, awaa240. <https://academic.oup.com/brain/article-pdf/doi/10.1093/brain/awaa240/33471792/awaa240.pdf> accessed 17 July 2020.
Meng H et al., CT imaging and clinical course of asymptomatic cases with COVID-19 pneumonia at admission in Wuhan, China. J Infect. 2020 Apr 12;S0163-4453(20)30211-5. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7152865/pdf/main.pdf> accessed 5 June 2020.
[125] [1963] AC 758.
[128] (23rd September 2016, Liverpool County Court).
[130] Esther Addley and Jim Waterson, ‘Sleep and exercise down, back pain and TV up in UK lockdown’ (7 April 2020 The Guardian) <https://www.theguardian.com/lifeandstyle/2020/apr/07/sleep-and-exercise-down-back-pain-and-tv-up-in-uk-lockdown> accessed 14 May 2020.
[131] ‘Burn-out an "occupational phenomenon": International Classification of Diseases’ (28 May 2019 WHO) <https://www.who.int/mental_health/evidence/burn-out/en/> accessed 14 August 2020.
[132] ‘BURNING THE CANDLE: STRATEGIES TO COMBAT WORKPLACE BURNOUT’ (2020 Robert Walters) <https://www.robertwalters.co.uk/content/dam/robert-walters/country/united-kingdom/files/whitepapers/Burning%20the%20candle%20-%20a%20guide%20to%20preventing%20workplace%20burnout.pdf> accessed 14 August 2020.
[133] Virtual parliamentary proceedings cause spike in injuries for interpreters: union’ (8 May 2020 CTV News) <https://www.ctvnews.ca/canada/virtual-parliamentary-proceedings-cause-spike-in-injuries-for-interpreters-union-1.4930398> accessed 12 May 2020.
[134] Federal interpreters suffer 'acoustic shock,' other concussion-like symptoms’ (CBC) <https://www.cbc.ca/news/canada/ottawa/federal-interpreters-raise-alarm-on-hearing-problems-1.5021258> accessed 12 May 2020.
[135] Max, ‘When A Corded Phone Is Superior To A Cordless’ (5 October 2014 liGo) <https://www.ligo.co.uk/blog/corded-phone-superior-cordless/> accessed 18 May 2020.
[136] ‘Legionella risks during the coronavirus outbreak’ (10 May 2020 HSE) <https://www.hse.gov.uk/news/legionella-risks-during-coronavirus-outbreak.htm> accessed 20 May 2020.
[137] Ministry of Justice, ‘Civil Justice Statistics Quarterly, England and Wales, October to December 2019 (provisional)’ (5 March 2020 GOV.UK) <https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/870184/civil-justice-statistics-quarterly-Oct-Dec.pdf> accessed 14 May 2020.
[138] Ministry of Justice, ‘Legal Aid, Sentencing and Punishment of Offenders Act 2012: Post-Legislative Memorandum’ (October 2017 GOV.UK) <https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/655971/LASPO-Act-2012-post-legislative-memorandum.pdf> accessed 14 May 2020.
[139] Neil Rose, ‘Number of motor claims stays low over last three months’ (20 October 2020 Litigation Futures) <https://www.litigationfutures.com/news/number-of-motor-claims-stays-low-over-last-three-months> accessed 21 December 2020.
[140] ‘Claims Portal Executive Dashboard’ (17 December 2020 Claims Portal) <https://www.claimsportal.org.uk/media/3131/eld-dashboard-november-2020.xlsm> accessed 21 December 2020.
[141] Neil Rose, ‘S&G to “automate everything” as it says: The future is digital”’ (2 October 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/sg-to-automate-everything-as-it-says-the-future-is-digital> accessed 14 December 2020.
[142] Nick Hilborne, ‘Big personal injury firms “to merge as market shrinks”’ (23 September 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/big-personal-injury-firms-to-merge-as-market-shrinks> accessed 14 December 2020.
[143] Neil Rose, ‘PI solicitors keen to maintain some remote hearings post-Covid’ (2 November 2020 Litigation Futures) <https://www.litigationfutures.com/news/pi-solicitors-keen-to-maintain-some-remote-hearings-post-covid> accesse 20 December 2020.
[144] Neil Rose, ‘It’s official: Whiplash reforms delayed by five months’ (27 February 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/its-official-whiplash-reforms-delayed-by-five-months?> accessed 2 March 2020.
[145] John Hyde, ‘Whiplash reforms delayed as MoJ removes claimants' safety net’ (27 February 2020 Law Gazette) <https://www.lawgazette.co.uk/whiplash-reforms-delayed-as-moj-removes-claimants-safety-net/5103237.article> accessed 13 May 2020.
[146] John Hyde, ‘Whiplash reforms delayed again - this time to April 2021’ (21 April 2020 Law Gazette) <https://www.lawgazette.co.uk/news/whiplash-reforms-delayed-again-this-time-to-april-2021/5103961.article> accessed 18 May 2020.
Neil Rose, ‘Whiplash reforms delayed until April 2021’ (21 April 2020 Legal Futures) https://www.legalfutures.co.uk/latest-news/whiplash-reforms-delayed-until-april-2021> accessed 18 May 2020.
[147] Nick Hilborne, ‘Consumers “growing in confidence” to manage own PI claims’ (26 October 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/consumers-growing-in-confidence-to-manage-own-pi-claims> accessed 21 December 2020.
[148] Neil Rose, ‘Leading PI firm declares: We’re ready for whiplash reforms’ (29 October 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/leading-pi-firm-declares-were-ready-for-whiplash-reforms> accessed 22 December 2020.
[149] John Hyde, ‘Insurers and claimant lawyers strike rare pact to stop PI reform’ (2 March 2020 Law Gazette) <https://www.lawgazette.co.uk/news/insurers-and-claimant-lawyers-strike-rare-pact-to-stop-pi-reform/5103295.article> accessed 18 May 2020.
[150] John Hyde, ‘Questions still linger over RTA Portal months before April lift-off’ (11 December 2020 Law Gazette) <https://www.lawgazette.co.uk/news/questions-still-linger-over-rta-portal-months-before-april-lift-off/5106781.article> accessed 21 December 2020.
[151] Neil Rose, ‘Still no rules but full steam to April for whiplash reforms, says MoJ’ (24 November 2020 Legal Futures) <https://www.legalfutures.co.uk/latest-news/still-no-rules-but-full-steam-to-april-for-whiplash-reforms-says-moj> accessed 22 December 2020.
[152] John Hyde, ‘MoJ still “mad keen” on expanded fixed costs regime, says expert’ (13 July 2020 Law Gazette) <https://www.lawgazette.co.uk/law/moj-still-mad-keen-on-expanded-fixed-costs-regime-says-expert/5104960.article> accessed 15 December 2020.
[153] ‘Personal injury lawyers announce legal action over discount rate’ (11 December 2020 Irish Legal) <https://www.irishlegal.com/article/personal-injury-lawyers-announce-legal-action-over-discount-rate> accessed 20 December 2020.
[154] <https://hansard.parliament.uk/Lords/2020-09-03/debates/7FB95A5D-E3D1-4577-A22F-2E597833DA2A/FatalAccidentsAct1976(Remedial)Order2020> accessed 14 December 2020.
[155] ‘Liability for NHS Charges (Treatment of Industrial Disease) (Scotland) Bill’ (The Scottish Parliament) <https://www.parliament.scot/parliamentarybusiness/CurrentCommittees/115777.aspx> accessed 20 August 2020.
[156] David Foskett, ‘FAQ: Guideline for Hourly Rates Survey (Courts and Tribunals Service) <https://www.judiciary.uk/related-offices-and-bodies/advisory-bodies/cjc/archive/costs-funding-and-third-party-funding/guideline-hourly-rates/ghrsurveyfaq/> accessed 20 April 2020.

































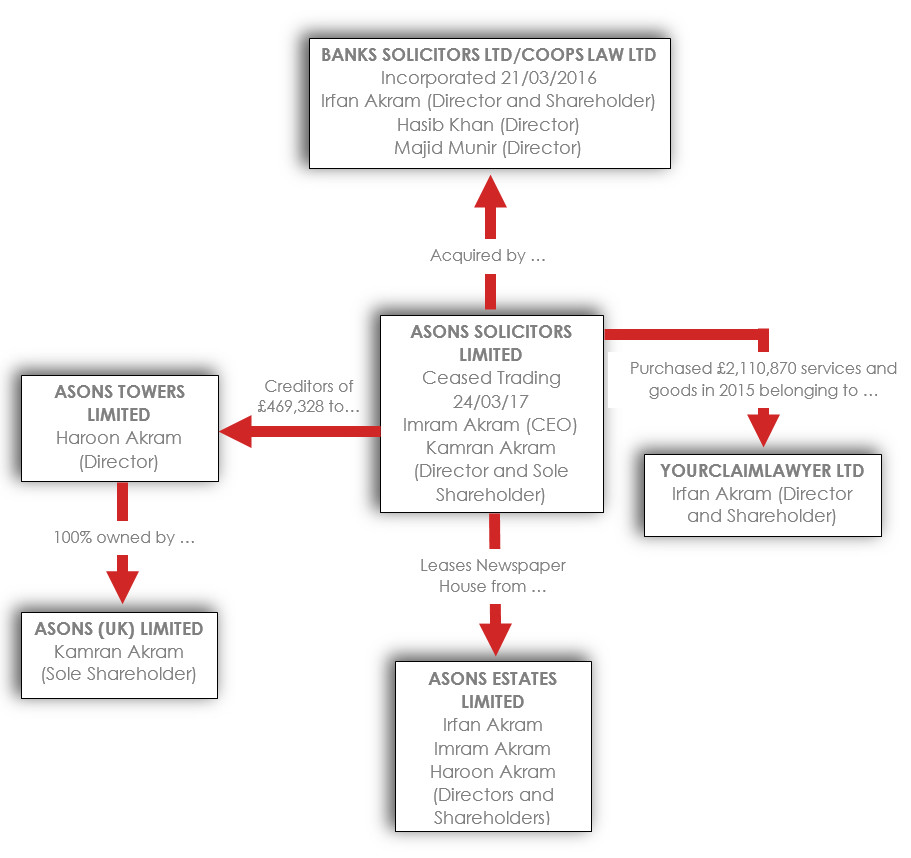
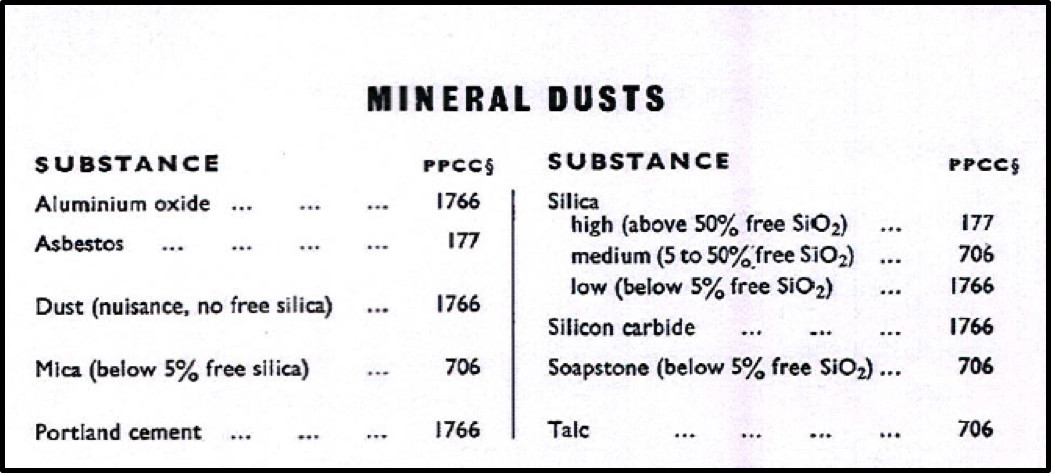
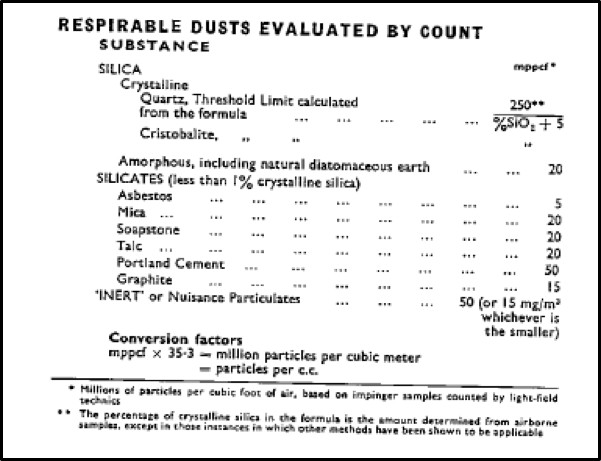

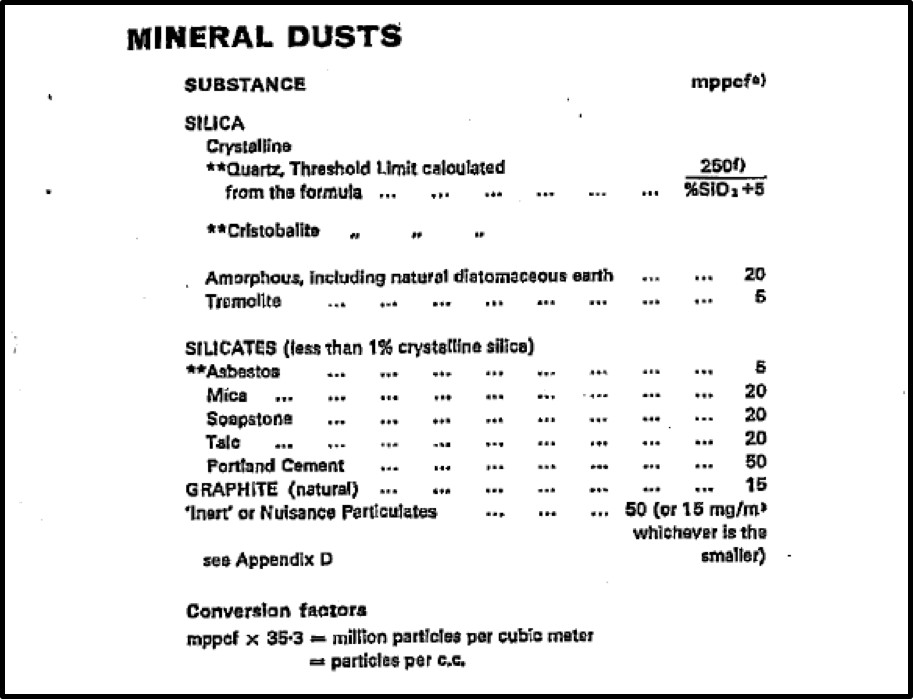

{kind=link}
{kind=link}
{kind=link}